
Lupus Stem Cell Therapy (HSCT): Life Changing Treatment for SLE

Medically reviewed by Dr. Rahul Bhargava, MBBS, MD (Medicine), DM (Clinical Haematology, AIIMS), Fellowship in Stem Cell Transplantation, Vancouver. Principal Director and Chief of HSCT, Haematology, Haemato-Oncology and Bone Marrow Transplantation, HSCT Hospital India.
Last reviewed: 11 July 2026. This guide cites peer-reviewed studies, which are linked throughout.
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease capable of involving virtually any organ system, and in a significant minority of patients it proves refractory to every available line of immunosuppressive therapy. For those patients, Hematopoietic Stem Cell Transplantation (HSCT) is opening a door that once felt firmly closed.
At HSCT Hospital India, a JCI-USA accredited centre, we have helped patients from Europe, North America and Australia get their lives back through HSCT treatment that is both world-class and carefully matched to each individual.
What Is Lupus?
Systemic lupus erythematosus is an autoimmune disease in which the immune system loses tolerance to the body’s own nuclear material. B lymphocytes produce autoantibodies directed against components of the cell nucleus, most characteristically double-stranded DNA. These autoantibodies bind their targets to form immune complexes, which deposit in tissue and activate the complement cascade, generating the inflammation that produces clinical disease.
This mechanism explains why lupus behaves as it does. Because nuclear material is present in every cell in the body, the immune complexes can deposit almost anywhere: in the glomeruli of the kidney, the synovium of the joints, the pleura and pericardium, the skin, the blood vessels and the central nervous system. Organ-specific autoimmune diseases attack one tissue. SLE attacks a molecular target that is universal, and the pattern of involvement can change over the course of the disease.
Disease activity in SLE is driven by ongoing autoantibody production and complement consumption, and this is why serological markers such as anti-double-stranded DNA titre and complement C3 and C4 levels are used to monitor patients. Rising anti-dsDNA with falling complement typically signals an impending flare.
SLE affects women approximately nine times more often than men, with peak incidence between the ages of 15 and 45. Prevalence and severity are both higher in patients of African, Hispanic and Asian ancestry.
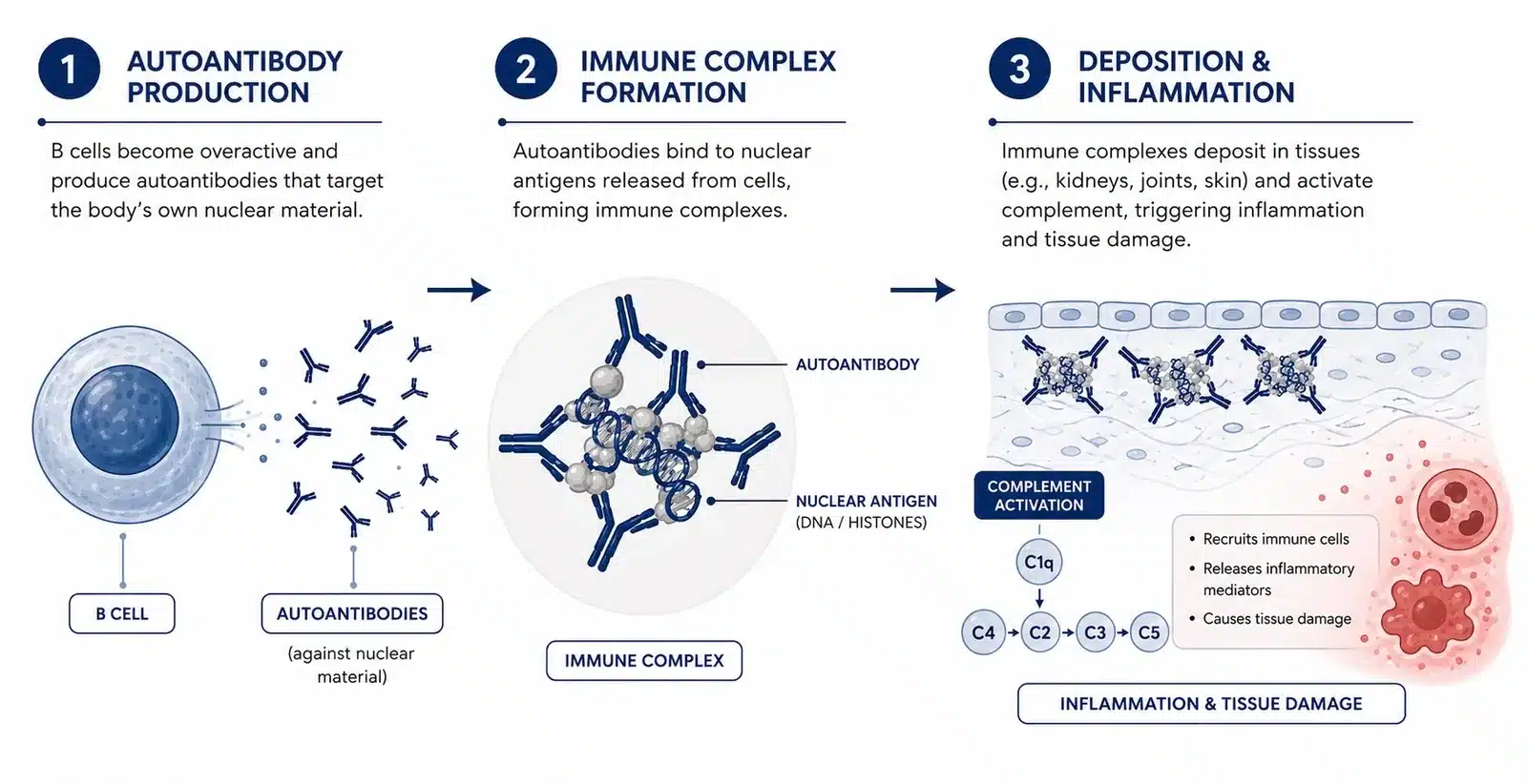
Figure 1. How lupus develops: autoantibody production, immune complex formation, and deposition in tissue leading to complement activation and inflammation.
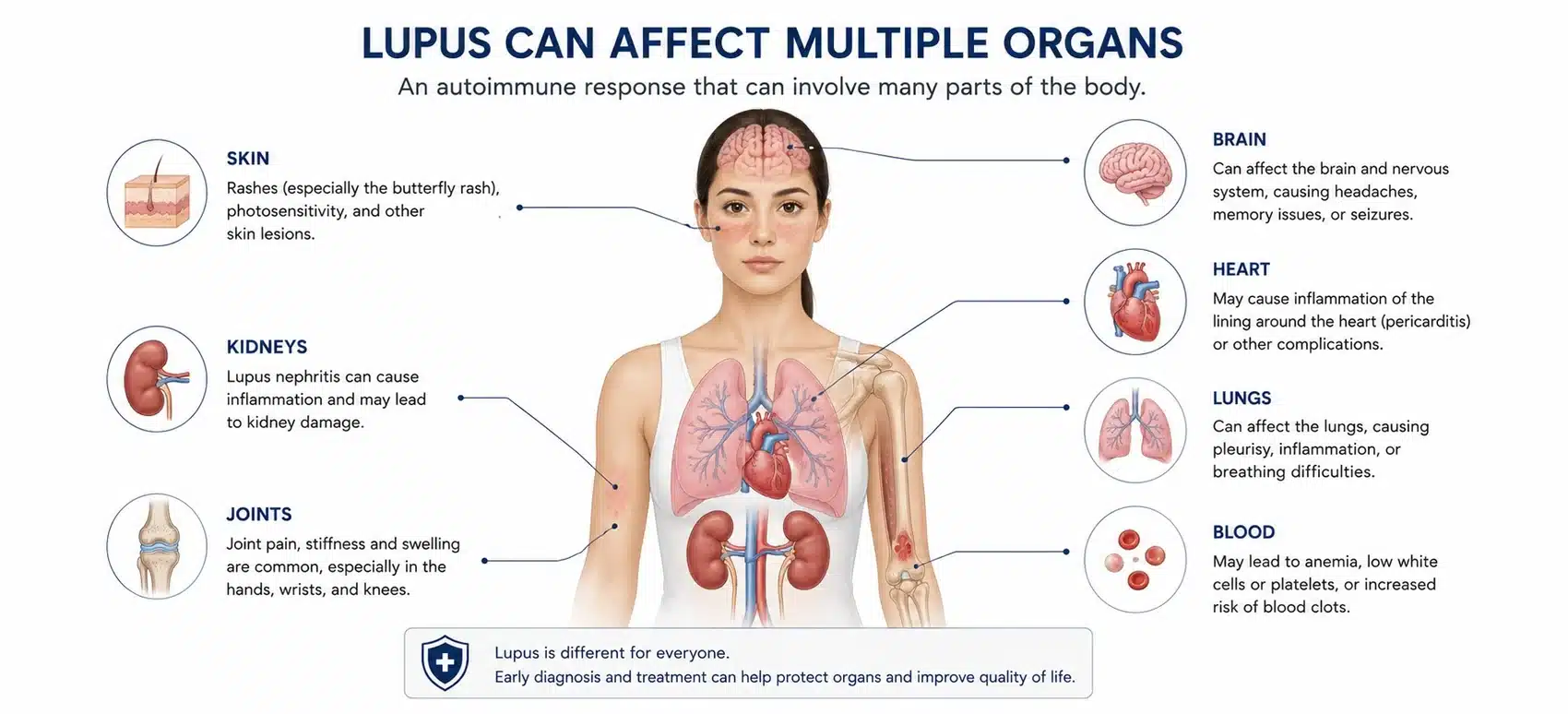
Figure 2. Systemic lupus erythematosus can involve the skin, joints, kidneys, heart, lungs, blood and central nervous system.
What Are the Symptoms of Lupus?
The clinical presentation of SLE varies widely between patients, reflecting the range of organ systems that may be involved. The most frequently reported features are:
- Constitutional: profound fatigue unrelieved by rest, fever in the absence of infection, and weight loss
- Musculoskeletal: symmetrical inflammatory arthralgia and arthritis, typically affecting the small joints of the hands, wrists and knees, with morning stiffness
- Cutaneous: the malar or butterfly rash across the cheeks and bridge of the nose, discoid lesions, and photosensitivity in which rashes appear or worsen following ultraviolet exposure
- Mucosal: oral and nasopharyngeal ulceration, characteristically painless
- Serosal: pleuritic chest pain on deep inspiration, and pericarditis
- Renal: peripheral oedema, periorbital swelling, hypertension and frothy urine, indicating proteinuria and lupus nephritis
- Haematological: anaemia, leucopenia, lymphopenia and thrombocytopenia
- Vascular: Raynaud phenomenon, in which the digits blanch and then become cyanotic on cold exposure
- Neuropsychiatric: headache, cognitive impairment, mood disturbance, seizure and, less commonly, stroke or psychosis
- Alopecia: diffuse hair thinning, and scarring alopecia where discoid lesions involve the scalp
SLE characteristically follows a relapsing and remitting course. Periods of relative quiescence are interrupted by flares of disease activity, and it is during these flares that irreversible organ damage accumulates.
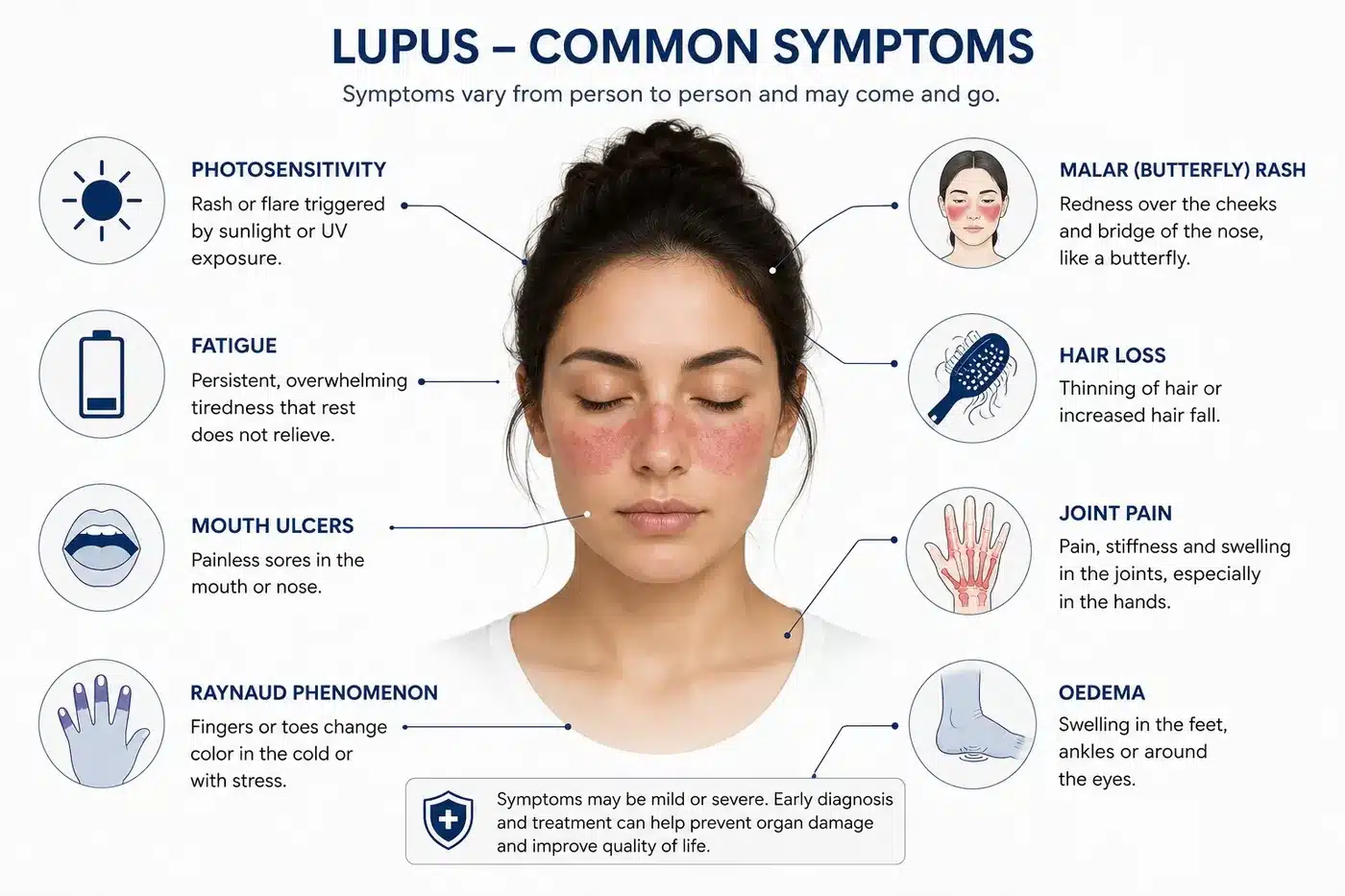
Figure 3. Common symptoms of systemic lupus erythematosus. Presentation varies considerably between patients.
How Is Lupus Diagnosed?
There is no single diagnostic test for systemic lupus erythematosus. Diagnosis rests on the combination of clinical features and serological findings, and classification is commonly guided by the 2019 EULAR and ACR criteria, which require a positive antinuclear antibody as the entry criterion.
The investigations used are as follows:
- Antinuclear antibody (ANA): positive in over 95% of patients with SLE. Its sensitivity is high but its specificity is poor, as a positive ANA is also found in other autoimmune conditions and in a proportion of healthy individuals.
- Anti-double-stranded DNA antibody: highly specific for SLE, and titres correlate with disease activity, particularly renal activity.
- Anti-Smith (anti-Sm) antibody: the most specific serological marker for SLE, though present in a minority of patients.
- Complement C3 and C4: consumed during active disease. Falling complement with rising anti-dsDNA is a recognised harbinger of flare.
- Antiphospholipid antibodies: lupus anticoagulant, anticardiolipin and anti-beta-2 glycoprotein I, which identify patients at elevated risk of thrombosis and pregnancy morbidity.
- Urinalysis and urine protein-to-creatinine ratio: to detect proteinuria and active urinary sediment, the earliest indicators of lupus nephritis.
- Renal biopsy: indicated where there is evidence of significant renal involvement, and used to establish the histological class of lupus nephritis, which determines treatment.
- Full blood count, renal function and inflammatory markers: to identify cytopenias and organ impairment.
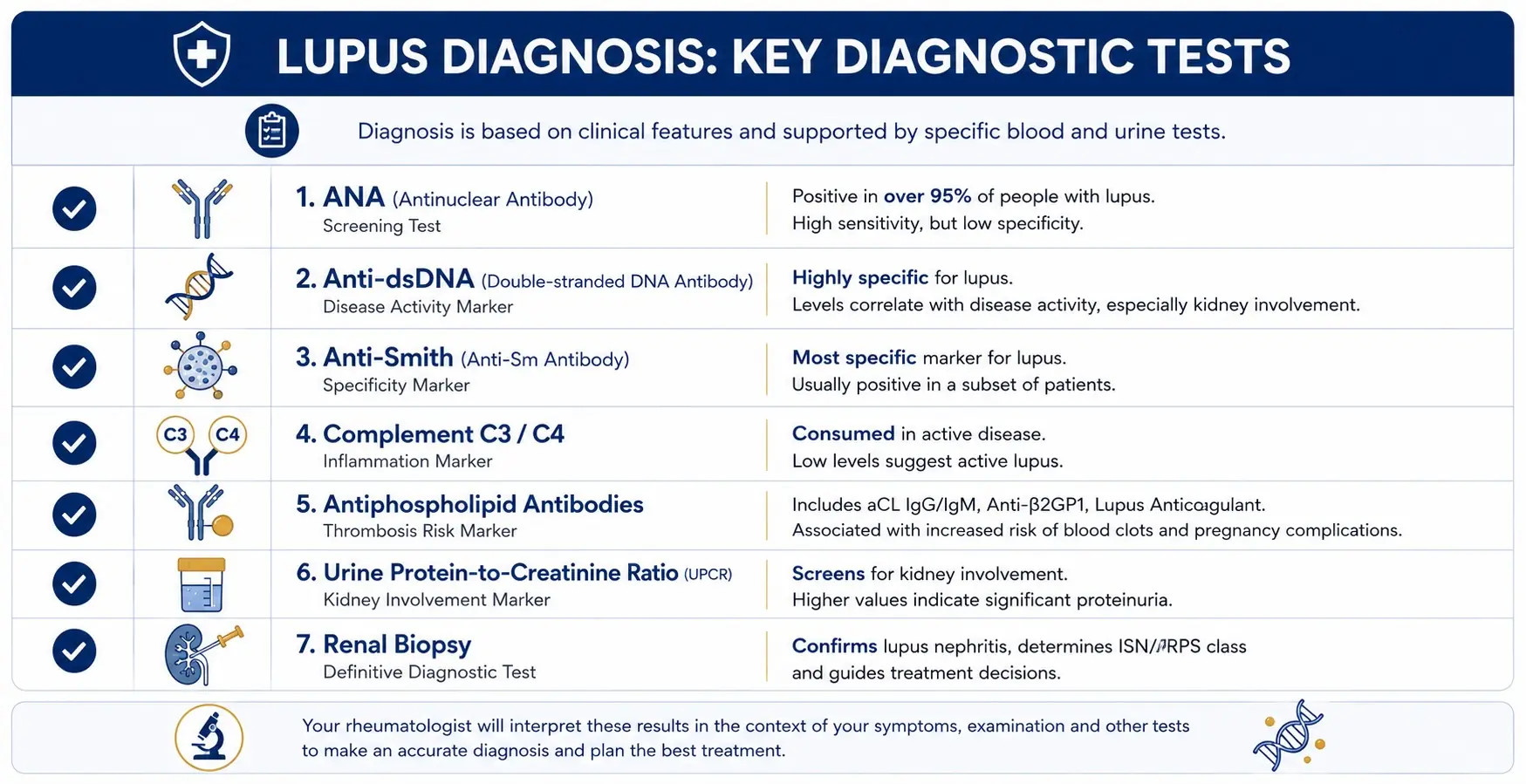
Figure 4. The key diagnostic tests used in systemic lupus erythematosus.
Disease activity is quantified using validated indices, most commonly the SLE Disease Activity Index (SLEDAI). Accrued, irreversible organ damage is measured separately, using the SLICC damage index. This distinction between activity and damage is fundamental to lupus management and to the assessment of candidates for transplantation.
What Triggers Lupus?
SLE arises where genetic susceptibility meets an environmental trigger. Multiple susceptibility loci have been identified, many involving genes that regulate interferon signalling, immune complex clearance and B cell activation, but no single gene causes the disease.
Recognised triggers include:
- Ultraviolet light, which induces apoptosis in keratinocytes and exposes nuclear antigens to the immune system, and is the best characterised trigger of cutaneous and systemic flare
- Infection, particularly Epstein-Barr virus, which is implicated through molecular mimicry
- Medications, including hydralazine, procainamide and certain anti-tumour necrosis factor agents, which can induce a drug-related lupus that typically resolves on withdrawal
- Hormonal factors, including oestrogen exposure and pregnancy, consistent with the marked female predominance of the disease
- Physical or psychological stress
Lupus is not attributable to diet, lifestyle or patient behaviour.
Is Lupus Progressive? Will It Get Worse?
The course of SLE varies considerably between patients. In the majority, disease is adequately controlled on standard therapy, flares become less frequent over time, and the long-term outlook is good. Ten-year survival in SLE now exceeds 90% in most published cohorts, a substantial improvement on historical figures.
In a smaller group, the disease is refractory. Flares recur despite escalating immunosuppression, and each flare deposits further irreversible damage. Disease activity and accrued damage are assessed separately in lupus. Activity can be suppressed. Damage cannot be reversed.
Approximately 40% to 50% of patients with SLE develop lupus nephritis, in which immune complexes deposit within the glomeruli of the kidney. Lupus nephritis treatment usually requires high-dose corticosteroid combined with mycophenolate mofetil or cyclophosphamide. Of those who develop proliferative nephritis, a significant proportion progress to end-stage renal disease despite treatment. Renal involvement remains a principal determinant of mortality in lupus, alongside cardiovascular disease and infection.
In refractory disease, therefore, delay carries a measurable cost in accrued organ damage.
What Are the Stages of Lupus?
SLE is not staged numerically in the manner of malignancy. Clinicians describe the disease in terms of activity, organ involvement and response to therapy. In practice, patients fall into four broad categories:
- Mild disease. Cutaneous and musculoskeletal involvement with constitutional symptoms, and no major organ threat. Managed with antimalarials, with short courses of low-dose corticosteroid as required.
- Moderate disease. More extensive skin and joint involvement, often with haematological abnormality such as thrombocytopenia. Requires corticosteroids with the addition of an immunosuppressant.
- Severe or organ-threatening disease. Involvement of the kidneys, central nervous system, heart or lungs. Treated with high-dose corticosteroid and intensive immunosuppression, most often mycophenolate mofetil or cyclophosphamide.
- Refractory disease. Disease activity persists despite corticosteroids, conventional immunosuppressants and biologic therapy. Refractory disease is the indication for which autologous HSCT is considered.
Where the kidneys are involved, lupus nephritis is classified histologically on renal biopsy according to the International Society of Nephrology and Renal Pathology Society (ISN/RPS) system.
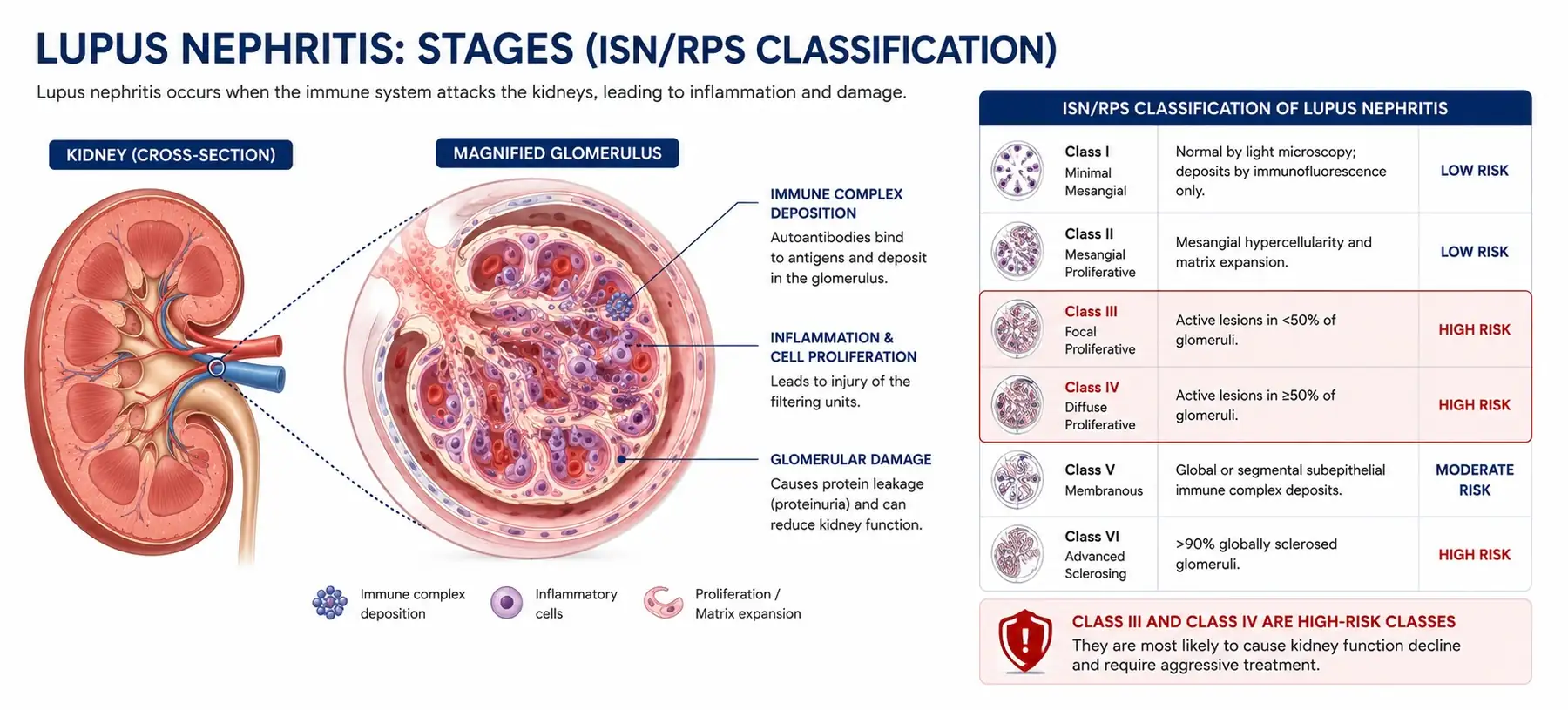
Figure 5. Lupus nephritis: immune complex deposition within the glomerulus, and the ISN/RPS histological classification.
| Class | Histology | Clinical significance |
|---|---|---|
| Class I | Minimal mesangial | Excellent renal prognosis |
| Class II | Mesangial proliferative | Good prognosis; rarely progresses |
| Class III | Focal proliferative | Significant risk of progression. Requires intensive immunosuppression. Commonly refractory. |
| Class IV | Diffuse proliferative | The most severe class. Highest risk of end-stage renal disease. The class most frequently seen in patients referred for HSCT. |
| Class V | Membranous | Nephrotic syndrome; thrombotic risk |
| Class VI | Advanced sclerosing | Irreversible scarring. Immunosuppression is not beneficial, and HSCT is not indicated. |
Table 1. ISN/RPS histological classification of lupus nephritis.
Class III and Class IV disease, described as focal and diffuse proliferative nephritis respectively, carry the greatest risk of progression to renal failure and are the classes most likely to prove refractory to conventional treatment. Class VI represents established scarring rather than active inflammation, and transplantation is not indicated.
Is Lupus the Same as MS?
No, although the two conditions share a common underlying mechanism, and both are treated at HSCT Hospital India with the same autologous transplant protocol.
In multiple sclerosis, the immune system attacks the myelin sheath surrounding nerve fibres within the central nervous system, and the resulting deficit is neurological: mobility, vision, coordination and bladder function. In systemic lupus erythematosus, autoantibodies and immune complexes attack connective tissue and multiple organ systems, and the resulting deficit may be renal, cardiac, pulmonary, haematological or neuropsychiatric.
What the two conditions share is the fault that drives them: a self-reactive immune repertoire that will continue to attack host tissue for as long as it exists. Conventional therapy suppresses that repertoire. It does not remove it. That shared mechanism is precisely why autologous haematopoietic stem cell transplantation, which ablates the repertoire and permits its reconstitution, is effective across both diseases.
What Happens If Lupus Goes Untreated?
Inadequately controlled SLE carries substantial risk of irreversible organ damage. The principal complications are:
- Renal: lupus nephritis progressing to end-stage renal disease, requiring dialysis or renal transplantation
- Cardiovascular: pericarditis, myocarditis, Libman-Sacks endocarditis, and markedly accelerated atherosclerosis. Cardiovascular disease is a leading cause of late mortality in lupus, and the risk is compounded by cumulative corticosteroid exposure.
- Pulmonary: pleuritis, pneumonitis, interstitial lung disease and pulmonary hypertension
- Neuropsychiatric: seizure, cerebrovascular accident, transverse myelitis, psychosis and persistent cognitive impairment
- Haematological: severe cytopenias, including autoimmune haemolytic anaemia and immune thrombocytopenia
- Thrombotic: arterial and venous thrombosis, and recurrent pregnancy loss, where antiphospholipid antibodies are present
- Infective: serious infection, driven both by the disease itself and by the intensity of the immunosuppression used to control it. Infection remains a leading cause of death in SLE.
In systemic lupus erythematosus, disease activity left unchecked converts progressively into permanent organ damage. Refractory disease is therefore treated aggressively rather than expectantly.
Standard Lupus Treatments
Most patients begin with one or more of the established therapies. Each suppresses immune activity rather than correcting the underlying autoimmunity.
- Antimalarials (hydroxychloroquine): the backbone of long-term management, reducing flare frequency, limiting damage accrual and improving survival. Recommended for essentially all patients with SLE in the absence of contraindication.
- Corticosteroids (such as prednisolone): rapidly effective in suppressing inflammation during a flare. Their limitation is cumulative toxicity, which includes osteoporosis and avascular necrosis, diabetes, hypertension, cataract, and a substantially elevated risk of serious infection. Minimising cumulative steroid exposure is a central objective of modern lupus care.
- Immunosuppressants: mycophenolate mofetil and cyclophosphamide are the agents of choice in proliferative lupus nephritis, with azathioprine and methotrexate used in less severe disease. Cyclophosphamide carries a dose-dependent risk of infertility and of secondary malignancy.
- Biologic therapies: belimumab targets B lymphocyte stimulator and is licensed in active SLE. Rituximab depletes CD20-positive B cells and is used off-licence in refractory disease. Anifrolumab targets the type I interferon receptor. Each is effective in a proportion of patients, and none is effective in all.
These treatments control disease effectively in many patients, and where they remain effective they should be continued. Autologous HSCT is not indicated in well-controlled lupus.
They are not, however, curative. Each suppresses immune function only for as long as it is administered, and the autoreactive immune repertoire driving the disease persists beneath that suppression. A significant number of patients cycle through successive agents, and some eventually find that these therapies stop working as well as they once did. For those patients, it is worth having a serious conversation about HSCT.
Can HSCT Treat Lupus? What the Evidence Shows
Yes, and for patients who have not responded to conventional therapy, it can be genuinely life-changing. Lupus stem cell therapy, properly termed autologous HSCT, is not an experimental intervention. A stem cell transplant for lupus has been studied for more than two decades, is supported by substantial published data, and is performed in accredited transplant centres worldwide.
HSCT does not suppress the immune system for a period. It resets it. Immunoablative conditioning eliminates the autoreactive lymphocyte population driving the disease, and the reinfused haematopoietic stem cells reconstitute an immune repertoire that no longer recognises host nuclear antigens as a target. Studies of immune reconstitution following transplantation have demonstrated a genuine renewal of the T cell repertoire, with restoration of regulatory T cell populations and normalisation of autoantibody titres.
The published outcomes are as follows:
- In the Northwestern University series led by Professor Richard K. Burt, 50 patients with severe, treatment-refractory SLE achieved a five-year overall survival of 84%, with disease-free survival at five years of 50%. The non-myeloablative protocol pioneered by Professor Burt is the protocol used at HSCT Hospital India. (Burt et al, JAMA)
- The European Society for Blood and Marrow Transplantation (EBMT) registry, the largest such dataset in the world, reports a comparable figure of approximately 50% disease-free survival at five years.
- In the EBMT and EULAR registry analysis, 66% of evaluable patients achieved remission, defined as a SLEDAI score below 3, within six months of transplantation. Approximately one third of those patients subsequently relapsed. (Jayne et al, Lupus)
- In long-term follow-up, sustained complete remission has been documented for a median in excess of 13 years following a single transplant. (Long-term follow-up study)
- Serological remission accompanies clinical remission in the majority of responders, with reversion of anti-double-stranded DNA to negative and normalisation of complement.
| Study | Patients | Key outcome |
|---|---|---|
| Northwestern University series | 50 | 84% five-year overall survival; 50% disease-free survival at five years |
| EBMT registry (largest worldwide dataset) | 85 | Approximately 50% disease-free survival at five years |
| EBMT / EULAR registry analysis | 53 | 66% achieved remission (SLEDAI below 3) within six months; approximately one third later relapsed |
| Long-term follow-up | – | Sustained complete remission documented beyond 13 years after a single transplant |
Table 2. Published outcomes of autologous HSCT in refractory systemic lupus erythematosus.
Every patient in these series had already exhausted conventional therapy, many facing progressive renal impairment and indefinite high-dose corticosteroid exposure. Against that natural history, an 84% five-year survival with a 50% drug-free remission rate represents a substantial change in prognosis.
How Does a Stem Cell Transplant for Lupus Work?
The treatment is autologous, meaning it uses the patient’s own haematopoietic stem cells. There is no donor, no requirement for tissue matching, and consequently no risk of graft-versus-host disease. The process takes place over approximately 30 days in hospital and proceeds in four stages.
- Mobilisation. Cyclophosphamide is administered, followed by granulocyte colony-stimulating factor, prompting the bone marrow to expand the haematopoietic stem cell population and release it into the peripheral bloodstream. The cyclophosphamide used at this stage also contributes to disease control in its own right.
- Harvest (Leukapheresis). The stem cells are collected from the peripheral blood by apheresis, in which blood is drawn from a vein, passed through a cell separator that isolates the CD34-positive stem cell fraction, and returned to the patient. The harvested cells are then cryopreserved and stored until required.
- Conditioning. A non-myeloablative, immunoablative regimen is administered, most commonly high-dose cyclophosphamide combined with anti-thymocyte globulin, which depletes the autoreactive lymphocyte population driving the disease, essentially making room for the new immune system to take hold. Non-myeloablative means the regimen is calibrated to ablate the immune system rather than the bone marrow itself, which is what distinguishes this protocol from transplantation for haematological malignancy and accounts for its substantially lower toxicity.
- Reinfusion. The patient’s own cryopreserved stem cells are thawed and reinfused. They migrate to the bone marrow and reconstitute a haematopoietic and immune system that, crucially, no longer recognises host tissue as a threat.
The protocol used at HSCT Hospital India requires no further chemotherapy or maintenance immunotherapy after discharge.
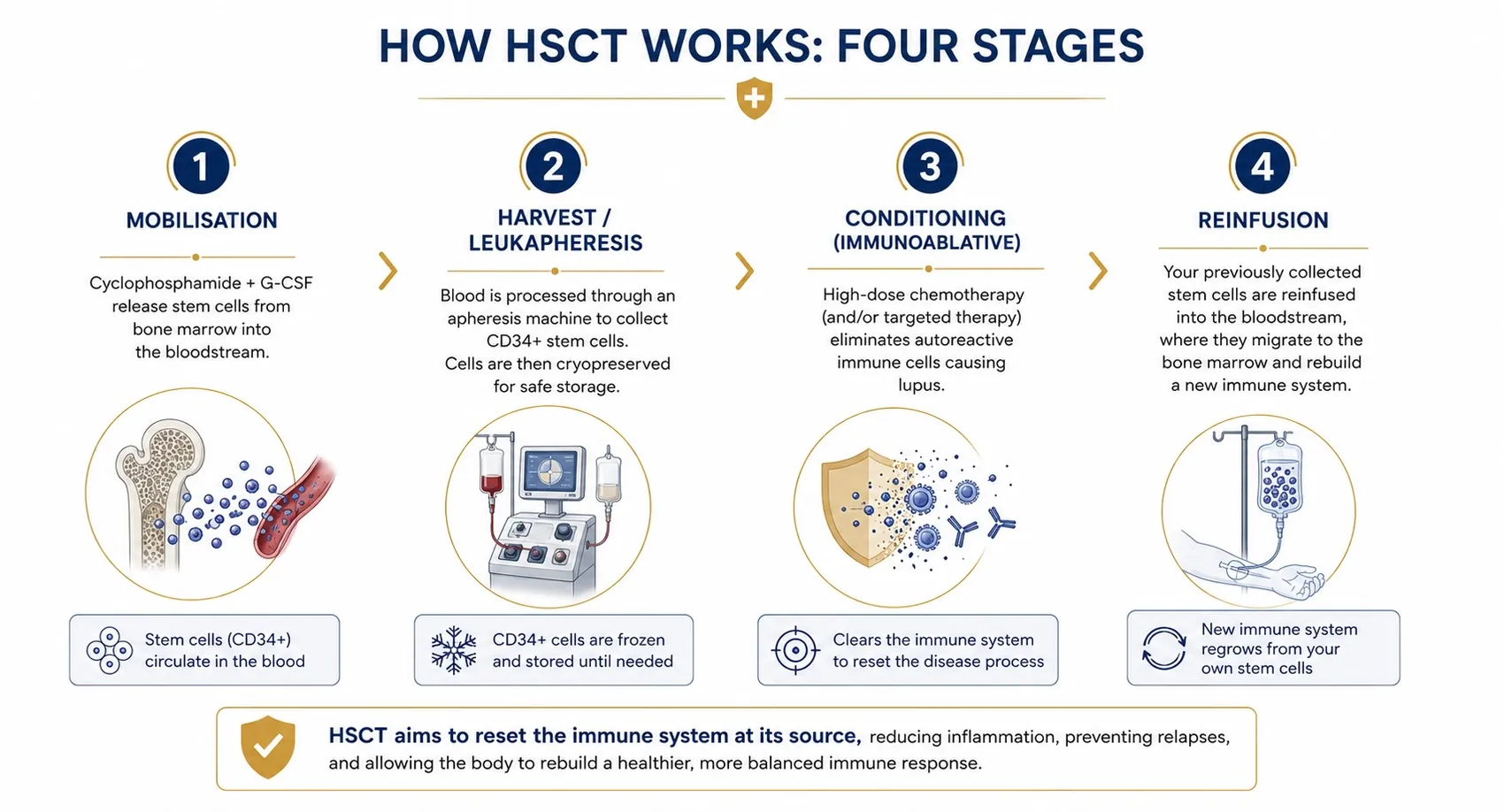
Figure 6. The four stages of autologous HSCT for lupus: mobilisation, harvest by leukapheresis, immunoablative conditioning, and reinfusion.
What Happens During the 30 Days in Hospital?
The admission follows a defined sequence, and patients are counselled through each phase before it begins.
- Days 1 to 5, evaluation. A full pre-transplant workup is completed on arrival: cardiac assessment by echocardiogram, pulmonary function testing, renal and hepatic function, infection screening, and a review of disease activity. Fertility preservation is discussed before any conditioning is given.
- Days 6 to 12, mobilisation and harvest. Cyclophosphamide and growth factor are administered, blood counts are monitored daily, and leukapheresis is performed once the peripheral CD34 count is adequate. The harvest itself is not painful and requires no anaesthetic.
- Days 13 to 18, conditioning. The immunoablative regimen is given. Nausea, fatigue and mucositis are common during this phase and are managed with supportive medication.
- Day 19, reinfusion. The stored stem cells are returned through a central line.
- Days 20 to 30, aplasia and engraftment. This is the period of greatest vulnerability. The white cell count falls to its nadir and the patient has minimal immune defence. Care is delivered in a deluxe private room with triple-level HEPA air filtration and 24-hour nursing. Neutropenic fever is anticipated and treated promptly with broad-spectrum antibiotics. Transfusion of red cells and platelets is given as required. Engraftment, marked by recovery of the neutrophil count, typically occurs within two to three weeks of reinfusion.
Patients are discharged once engraftment is established and they are clinically stable. Immune reconstitution continues over the following six to twelve months, during which vaccination schedules are repeated and infection precautions are maintained.
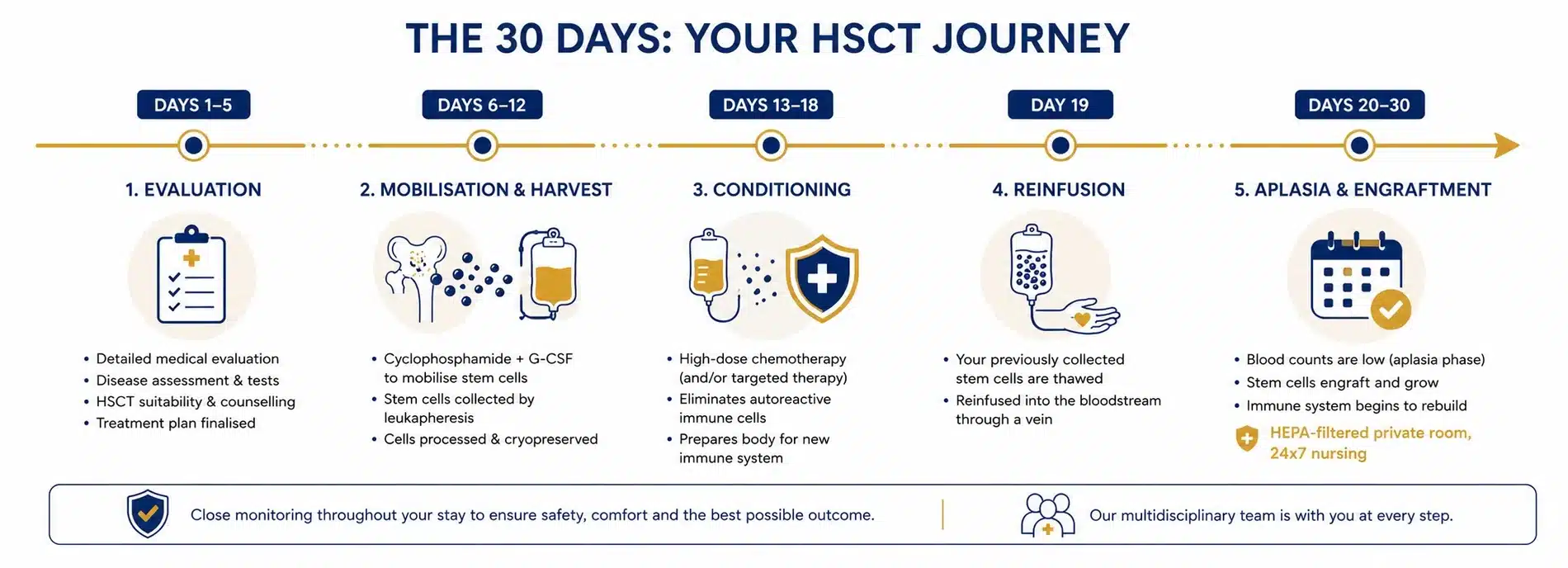
Figure 7. The 30 day in-hospital HSCT treatment timeline at HSCT Hospital India.
What Are the Risks of HSCT for Lupus?
Autologous HSCT is a serious intervention and the risks are discussed in full with every patient before any decision is taken.
- Infection. The principal risk. During the aplastic phase the patient has minimal neutrophil defence, and bacterial, fungal and viral infection can progress rapidly. This is the reason the entire admission is conducted as an inpatient in a HEPA-filtered transplant unit rather than on an outpatient basis.
- Transplant-related mortality. Reported at approximately 5% to 7% in the published lupus transplant series, and it is higher in patients with significant established organ damage, which is a principal reason for transplanting before end-organ failure supervenes.
- Cytopenias. Anaemia and thrombocytopenia during the aplastic phase, managed with transfusion.
- Mucositis, nausea and alopecia. Expected consequences of the conditioning regimen. Hair regrows following engraftment.
- Fertility. Cyclophosphamide is gonadotoxic and the regimen carries a real risk of infertility and premature ovarian insufficiency. Fertility preservation, by oocyte, embryo or sperm cryopreservation, is discussed with every patient of reproductive age before conditioning begins.
- Secondary autoimmunity. A minority of patients develop a new autoimmune phenomenon, most commonly thyroid disease, during immune reconstitution.
- Late effects. Long-term follow-up of transplanted patients monitors for secondary malignancy, a recognised though uncommon consequence of alkylating chemotherapy.
These risks are weighed against the natural history of refractory lupus, which in this population includes progressive renal failure, cumulative corticosteroid toxicity and a significant mortality of its own.
HSCT or CAR T Cell Therapy for Lupus?
Anti-CD19 CAR T cell therapy for lupus, also written CAR-T, is an emerging treatment in refractory systemic lupus erythematosus. In CAR-T therapy, the patient’s own T cells are genetically engineered to express a chimeric antigen receptor directed against CD19, a surface marker on B lymphocytes, and are reinfused to deplete the B cell population responsible for autoantibody production.
In the initial series reported by Schett and Mackensen at Erlangen, all five patients with refractory SLE achieved drug-free remission within three months of a single CAR-T cell infusion, with normalisation of anti-double-stranded DNA and complement. In a subsequent pooled analysis of 47 lupus patients treated across ten studies, 81% achieved a low disease activity state. Cytokine release syndrome occurred in the majority of patients, predominantly at grade 1 to 2 severity. (Pooled analysis of 47 patients across 10 studies)
Three factors nonetheless establish autologous HSCT as the appropriate treatment for the majority of refractory patients at present.
- Availability. Fewer than fifty patients with SLE worldwide have received CAR-T cell therapy. It is delivered in a small number of academic centres, almost exclusively within clinical trials carrying restrictive entry criteria. For the overwhelming majority of lupus patients, it is not an accessible option.
- Duration of follow-up. CAR-T in SLE is supported by approximately two years of follow-up data. Autologous HSCT is supported by more than twenty years, with documented remissions exceeding thirteen years. The durability of CAR-T remission is not yet established.
- Cost and access. CAR-T remains among the most expensive interventions in modern medicine. HSCT at HSCT Hospital India is provided as an all-inclusive package of 30,000 US dollars, with a waiting period measured in weeks.
| Autologous HSCT | Anti-CD19 CAR-T | Conventional therapy | |
|---|---|---|---|
| Mechanism | Immunoablation and reconstitution of the entire immune repertoire | Targeted depletion of CD19-positive B cells | Ongoing suppression of immune activity |
| Drug-free remission | Approximately 50% at five years | 81% low disease activity in pooled analysis | Not achieved; therapy is lifelong |
| Published follow-up | Over 20 years; remissions documented beyond 13 years | Approximately 2 years | Decades |
| Patients treated worldwide | Several hundred with SLE | Fewer than 50 with SLE | Standard of care |
| Availability | Accredited transplant centres; waiting period measured in weeks | A small number of academic centres, almost exclusively within clinical trials | Widely available |
| Principal risk | Infection during the aplastic phase; transplant-related mortality 5% to 7% | Cytokine release syndrome, predominantly grade 1 to 2 | Cumulative corticosteroid and immunosuppressant toxicity |
| Cost at HSCT Hospital India | 30,000 US dollars, all inclusive | Among the most expensive interventions in medicine | Lifelong drug cost |
Table 3. Autologous HSCT, anti-CD19 CAR T cell therapy and conventional immunosuppression compared in refractory SLE.
CAR-T cell therapy may well prove to be the future of treatment in refractory lupus, and any patient able to access a trial should give it serious consideration. For the majority of patients who cannot, autologous HSCT remains an established treatment supported by two decades of published evidence and available without delay.
Can Lupus Be Cured?
Conventional lupus therapy suppresses the immune system for as long as it is taken. Lupus stem cell therapy, in the form of autologous HSCT, is the only treatment shown to produce sustained remission in the absence of ongoing medication.
In published series, approximately half of transplanted patients remain in drug-free remission five years after a single course of treatment. Sustained complete remission has been documented beyond thirteen years, accompanied by reversion of anti-double-stranded DNA to negative and normalisation of complement.
A proportion of patients relapse and resume medication. Agents that had previously failed frequently regain their effectiveness following transplantation, a finding reported consistently across transplant series.
Who Is a Candidate for HSCT?
HSCT is not the right fit for every lupus patient, and we would never suggest it was. Eligibility is assessed carefully, and the decision is always made with patient safety at the centre. The key factors we look at include:
- A confirmed diagnosis of systemic lupus erythematosus meeting established classification criteria
- Severe disease refractory to standard therapy, generally including corticosteroids, conventional immunosuppressants such as mycophenolate mofetil or cyclophosphamide, and at least one biologic agent
- Serologically and clinically active disease, evidenced by elevated SLEDAI, raised anti-double-stranded DNA and complement consumption, rather than symptoms attributable predominantly to established organ damage
- Organ-threatening involvement, most commonly ISN/RPS Class III or Class IV lupus nephritis, carrying a poor long-term prognosis on conventional treatment
- Adequate cardiac, pulmonary, hepatic and renal reserve to tolerate the conditioning regimen, established by echocardiogram, pulmonary function testing and biochemistry
- Absence of active uncontrolled infection and of malignancy
- Age and general fitness
Patients with end-stage renal disease already established on dialysis, or with irreversible organ failure, are generally not candidates, because transplantation addresses active inflammation and cannot reverse damage already accrued. This is the clinical reason that referral before end-organ failure produces materially better outcomes.
At HSCT Hospital India, every potential patient goes through a full multi-disciplinary review before anything is decided. Our team will always give you an honest answer, even if that answer is that HSCT is not the right option for you right now.
What Does Lupus Treatment Cost?
The all-inclusive HSCT package at HSCT Hospital India is 30,000 US dollars. It covers a 30-day in-hospital admission for the patient and one attendant, in a deluxe private room equipped with HEPA filtration at triple level.
The package includes the full pre-transplant evaluation, mobilisation, leukapheresis and cryopreservation, the conditioning regimen, reinfusion, all consultant fees, investigations, medicines and consumables, transfusion support, physiotherapy, and food and laundry for both patient and attendant, together with airport transfers. No further chemotherapy is required following discharge.
| Country | Typical cost | Admission |
|---|---|---|
| India (HSCT Hospital India) | 30,000 US dollars | 30 days fully inpatient, patient and attendant, deluxe private room with triple-level HEPA filtration |
| Russia | 40,000 to 45,000 US dollars | 5 to 6 weeks, inpatient |
| Mexico | Approximately 54,500 US dollars | Largely outpatient, with accommodation near the clinic |
| Germany | Approximately 68,000 US dollars | 6 to 7 weeks, inpatient |
| United States | 150,000 to 200,000 US dollars | 6 to 7 weeks. For most lupus patients, available only within a clinical trial. |
Table 4. Indicative cost of autologous HSCT by country.
Not included: international airfare, and the management of any complication extending the admission beyond 30 days. These are set out in writing before any commitment is made.
Why Choose HSCT Hospital India for Life Changing Lupus Treatment
 HSCT Hospital India is one of the finest private hospitals in India and Accredited by JCI-USA. Most Affordable, 30,000 US $ HSCT package includes complete treatment cost for 30 days in hospital stay in a deluxe private room, Doctors Fee, Tests and Consultations, Medicines, Consumables, Physiotherapy and also Food and Laundry for both the patient and the attendant, Airport Transfers etc. Large number of patients from Europe, America and Australia already treated successfully. Click here to know more
HSCT Hospital India is one of the finest private hospitals in India and Accredited by JCI-USA. Most Affordable, 30,000 US $ HSCT package includes complete treatment cost for 30 days in hospital stay in a deluxe private room, Doctors Fee, Tests and Consultations, Medicines, Consumables, Physiotherapy and also Food and Laundry for both the patient and the attendant, Airport Transfers etc. Large number of patients from Europe, America and Australia already treated successfully. Click here to know more
 Complete 30 day HSCT done in hospital. Private deluxe rooms are very well served for patient and attendant comfort and equipped with HEPA Filter with Triple Level Air Filtration. No outside hospital stay avoids risk of infection during the aplastic phase, 24 x 7 nursing care and best medical attention. Advanced HSCT protocol used does not require any further chemo or treatment after leaving the hospital. Click here to get complete details
Complete 30 day HSCT done in hospital. Private deluxe rooms are very well served for patient and attendant comfort and equipped with HEPA Filter with Triple Level Air Filtration. No outside hospital stay avoids risk of infection during the aplastic phase, 24 x 7 nursing care and best medical attention. Advanced HSCT protocol used does not require any further chemo or treatment after leaving the hospital. Click here to get complete details
 International and Globally Renowned Accreditations. HSCT Hospital India is accredited by the Joint Commission International, USA, the National Accreditation Board for Hospitals and Healthcare Providers (NABH), and the National Accreditation Board for Laboratories (NABL) for processes and high quality patient care. Click here to know more
International and Globally Renowned Accreditations. HSCT Hospital India is accredited by the Joint Commission International, USA, the National Accreditation Board for Hospitals and Healthcare Providers (NABH), and the National Accreditation Board for Laboratories (NABL) for processes and high quality patient care. Click here to know more
 More than 1,500 patients from Europe, America and Australia have already been treated successfully at HSCT Hospital India. Our multi-disciplinary team reviews every lupus referral, including serology, renal histology and organ reserve, before any decision is taken. Click here to watch patient testimonial videos
More than 1,500 patients from Europe, America and Australia have already been treated successfully at HSCT Hospital India. Our multi-disciplinary team reviews every lupus referral, including serology, renal histology and organ reserve, before any decision is taken. Click here to watch patient testimonial videos
Related reading: HSCT for Multiple Sclerosis, HSCT for CIDP, HSCT for Myasthenia Gravis, HSCT for NMOSD.
Real Patient– Real Stories


