
Crohn’s Disease New Treatment (HSCT): Life Changing Stem Cell Transplant for Refractory Crohn’s
Medically reviewed by Dr. Rahul Bhargava, MBBS, MD (Medicine), DM (Clinical Haematology, AIIMS), Fellowship in Stem Cell Transplantation, Vancouver. Principal Director and Chief of HSCT, Haematology, Haemato-Oncology and Bone Marrow Transplantation, HSCT Hospital India.
Last reviewed: 13 July 2026. This guide cites peer-reviewed studies, which are linked throughout.
What Is Crohn’s Disease?
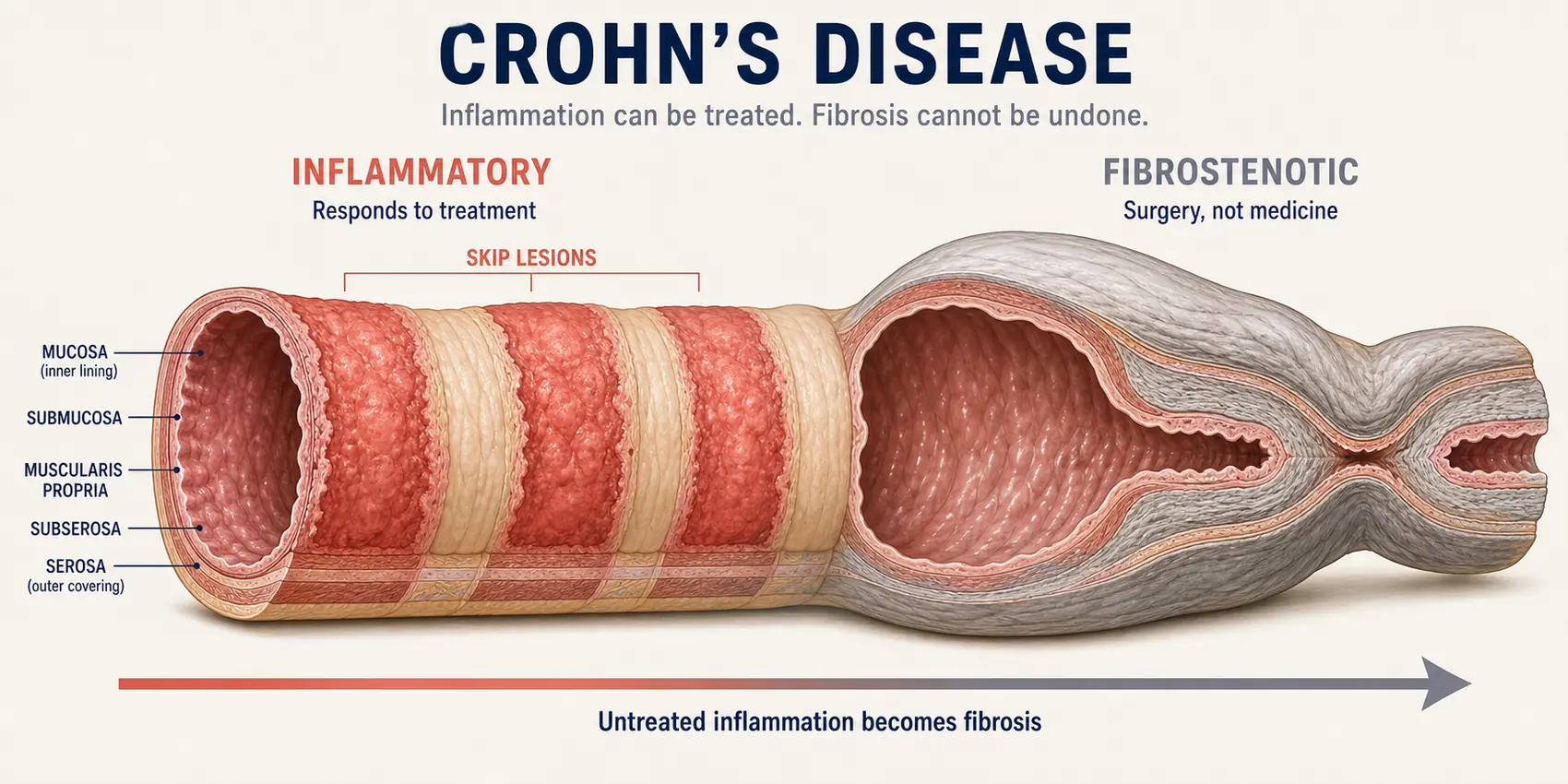
Crohn’s disease is a chronic inflammatory bowel disease in which the immune system attacks the wall of the digestive tract. It can affect any part of the gut from the mouth to the anus, though it most often involves the last part of the small intestine, the terminal ileum, and the first part of the colon. The inflammation is transmural, meaning it passes through the entire thickness of the bowel wall rather than staying at the surface. That single feature explains almost everything that follows in this guide.
Transmural inflammation does two things. In the short term it causes pain, diarrhoea, bleeding and urgency. Over the long term, the body responds to repeated inflammation the way it responds to any repeated injury: it lays down collagen. Collagen in the bowel wall becomes fibrosis, and fibrosis becomes a stricture, a fixed narrowing that no drug can reverse. Inflammation can also burrow outward through the wall and create a fistula, an abnormal tunnel between the bowel and another organ or the skin.
The distinction between inflammation and fibrosis runs through this entire guide, and it is the distinction that decides whether a stem cell transplant can help you. Inflammation is immune activity happening now. Fibrosis is the scar that yesterday’s inflammation left behind. Every treatment for Crohn’s disease, including HSCT, acts on inflammation. Nothing in medicine dissolves an established fibrotic stricture. That is why two patients with the same number of years of Crohn’s disease can have completely different answers to the question of whether transplantation will help them.
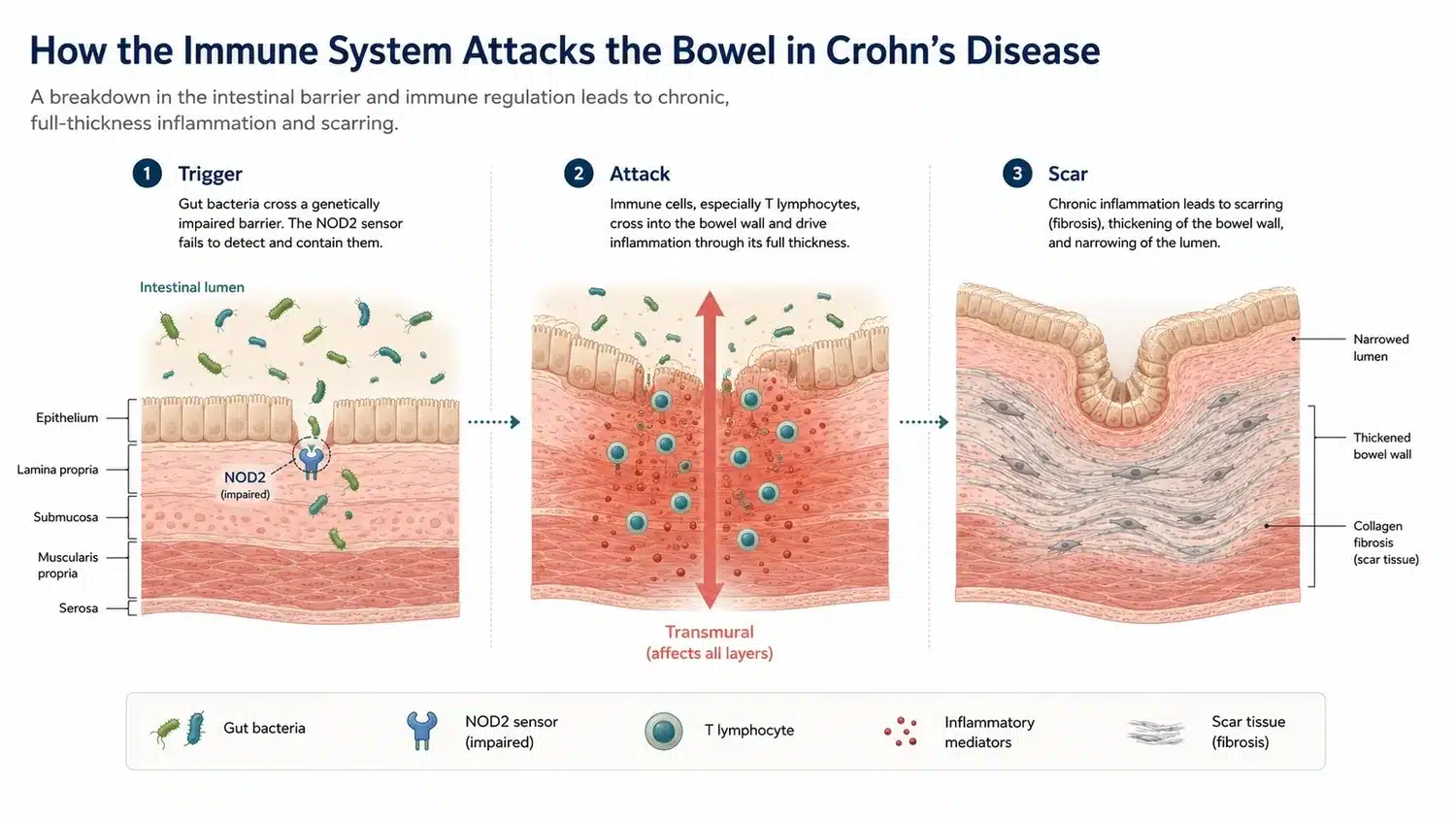
Figure 1. Transmural inflammation in Crohn’s disease, and its progression to fibrosis. Inflammation is reversible. Fibrosis is not.
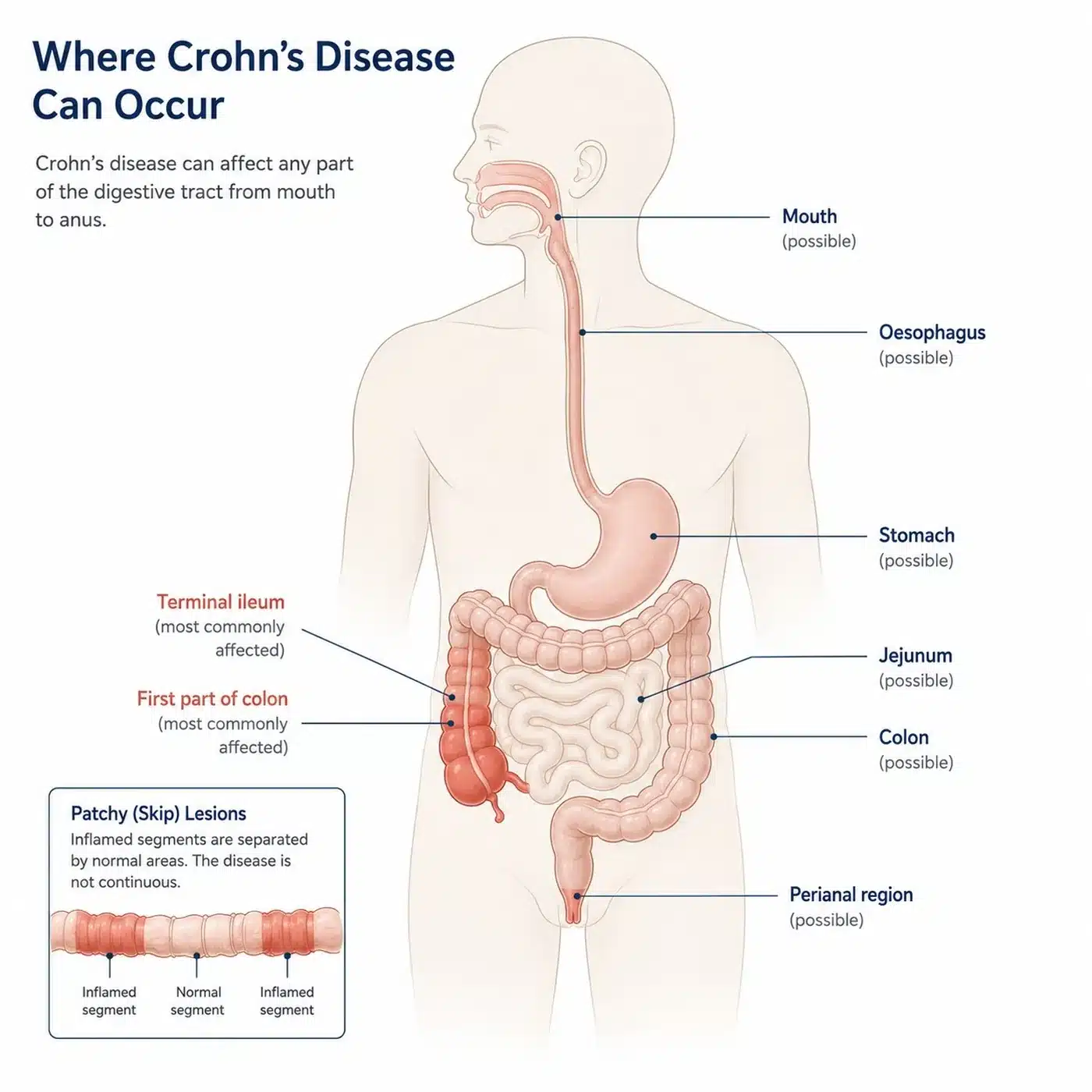
Figure 2. Crohn’s disease can occur anywhere from mouth to anus, in patchy skip lesions. The terminal ileum is the most common site.
What Are the Symptoms of Crohn’s Disease?
The most common symptoms of Crohn’s disease are persistent diarrhoea, cramping abdominal pain that is often worst in the lower right side, unintended weight loss, fatigue and blood in the stool. Many patients also have fever during a flare, and reduced appetite that compounds the weight loss.
Crohn’s disease is not confined to the gut. Extraintestinal manifestations affect up to two in five patients and include inflammatory arthritis of the large joints and the spine, episcleritis and uveitis in the eye, erythema nodosum and pyoderma gangrenosum in the skin, and primary sclerosing cholangitis in the bile ducts. These are not coincidental separate diseases. They are the same misdirected immune response appearing in a different tissue, which is one reason a treatment that resets the immune system as a whole is a rational approach.
Perianal disease deserves separate mention because it is common, it is disabling, and patients rarely raise it. Perianal fistulas and abscesses affect roughly one in three patients with Crohn’s disease at some point. They respond poorly to conventional therapy and they weigh heavily on quality of life. Perianal fistulising disease is one of the situations in which mesenchymal stromal cell therapy, which is a different treatment from HSCT, has an established role, and we set out that distinction later in this guide.
Symptoms alone are an unreliable guide to what is happening inside the bowel. A substantial proportion of patients with Crohn’s disease have ongoing symptoms driven by bile acid malabsorption, bacterial overgrowth or an irritable bowel overlay while their inflammation is actually quiescent. The reverse is also true: patients can have significant endoscopic ulceration while feeling reasonably well. This is why eligibility for transplantation is never decided on how a patient feels.
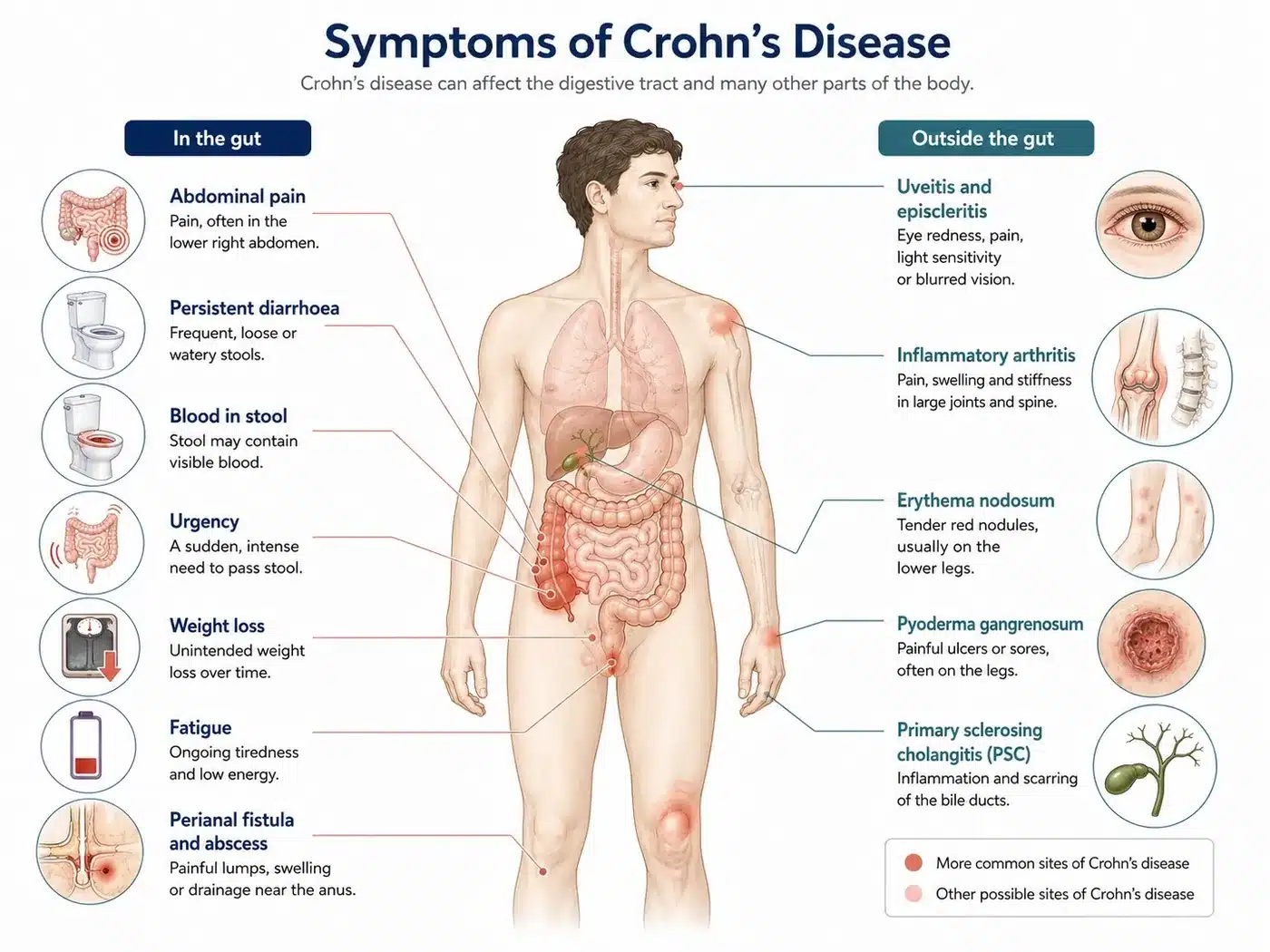
Figure 3. Crohn’s disease is not confined to the gut. Extraintestinal manifestations affect up to two in five patients.
How Is Crohn’s Disease Diagnosed?
Crohn’s disease is diagnosed by combining ileocolonoscopy with biopsy, cross-sectional imaging of the small bowel, and laboratory markers of inflammation. No single test makes the diagnosis. The colonoscopy shows the characteristic pattern of the disease: patchy skip lesions with normal mucosa in between, deep linear ulcers, and a cobblestone appearance. Biopsies may show granulomas, which are clusters of immune cells that are highly suggestive of Crohn’s disease though present in only a minority of specimens.
Two blood and stool markers matter more than any others. C-reactive protein, or CRP, is a general marker of inflammation in the body. Faecal calprotectin is a protein released by neutrophils into the stool and is a direct measure of inflammation in the bowel itself. Faecal calprotectin is the single most useful non-invasive test in Crohn’s disease because it separates a patient whose symptoms come from active inflammation from a patient whose symptoms come from a non-inflammatory cause. That separation is not academic. It is the difference between a patient who may benefit from immune reset and a patient who will not.
Cross-sectional imaging is what distinguishes inflammation from fibrosis, and it is therefore the most important investigation in a transplant assessment. Magnetic resonance enterography, or MRE, and intestinal ultrasound can both show whether a narrowed segment of bowel is thickened because it is inflamed or because it is scarred. An inflamed stricture enhances with contrast, shows oedema in the bowel wall and is often accompanied by a raised calprotectin. A fibrotic stricture is a fixed narrowing with little enhancement. The two look similar on a symptom questionnaire and completely different on an MRE.
This is where a formal transplant evaluation earns its place. A patient can be told for years that they have refractory Crohn’s disease when what they actually have is a fibrotic stricture causing obstructive symptoms in the absence of active inflammation. No amount of immunosuppression, and no transplant, will open that stricture. It needs a surgeon or an endoscopic dilatation. Establishing which of the two you have is the first thing we do.
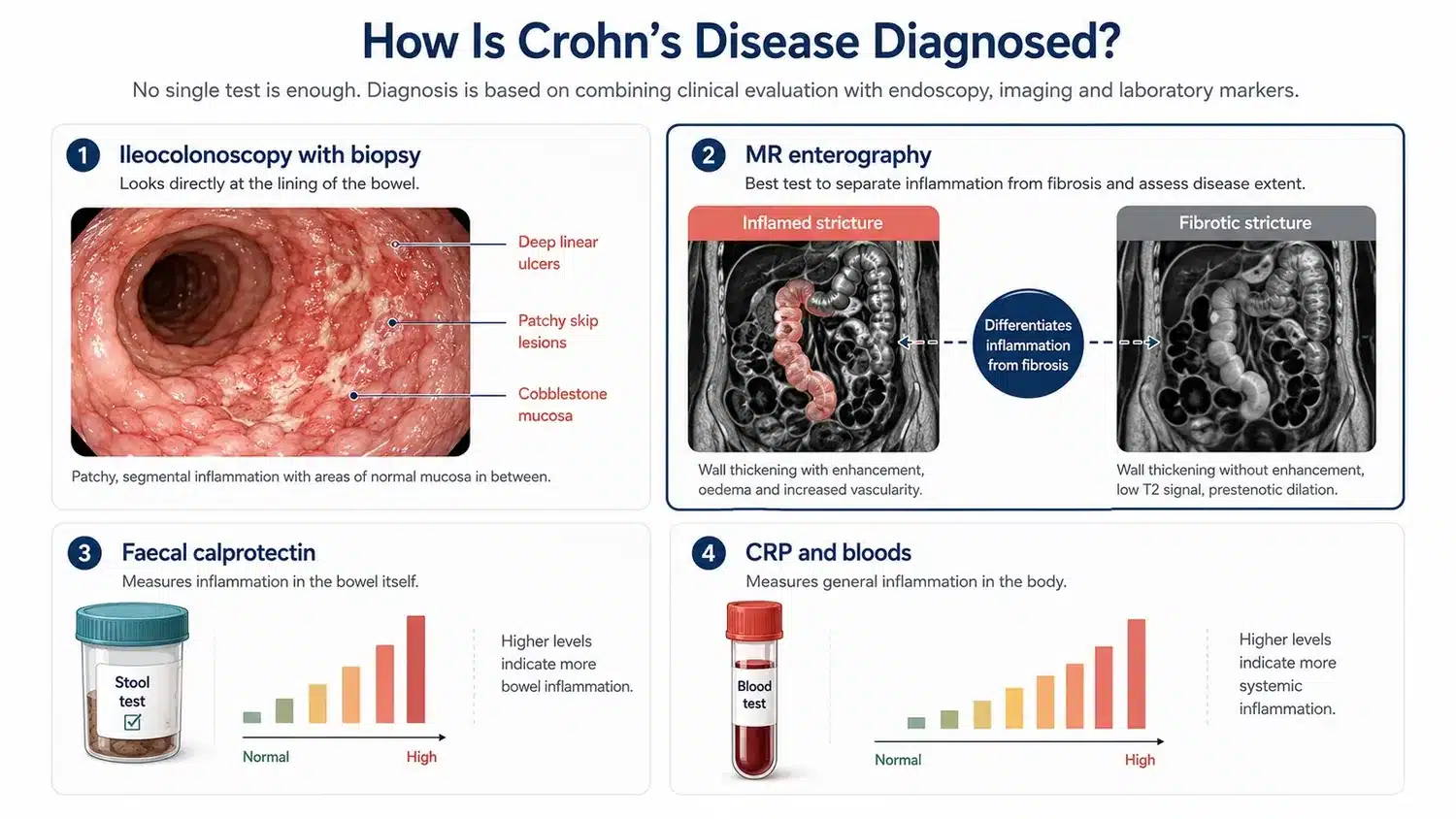
Figure 4. MR enterography is the investigation that separates an inflamed stricture from a fibrotic one. That distinction decides whether a transplant can help.
What Triggers Crohn’s Disease?
Crohn’s disease develops when a genetically susceptible person mounts an abnormal immune response to the bacteria that normally live in the gut. Over two hundred genetic loci have been associated with inflammatory bowel disease, the best characterised being NOD2, which encodes a protein that senses bacterial cell wall components. A defect in NOD2 impairs the ability of the innate immune system to handle ordinary gut bacteria, and the adaptive immune system compensates with a sustained inflammatory response against the intestinal wall.
Genetics alone do not cause the disease. Smoking roughly doubles the risk of developing Crohn’s disease and clearly worsens its course, which is one of the few genuinely modifiable factors and the single most useful thing a patient can act on. Antibiotic exposure, particularly in early life, a diet high in ultra-processed food, and a course of gastroenteritis have all been associated with subsequent diagnosis.
Crohn’s disease is not caused by anything the patient did, and it is not caused by stress, though stress reliably worsens symptoms once the disease is established. It is also not a food allergy, and no exclusion diet has been shown to induce durable remission in adults with established disease, though exclusive enteral nutrition does induce remission in children.
The reason the trigger matters clinically is that it explains why the disease relapses. The genetic susceptibility does not go away and the gut bacteria do not go away. What autologous HSCT changes is the third element, the aberrant adaptive immune response, and that is why remission after transplantation can be durable rather than temporary.
Is Crohn’s Disease Progressive? Will It Get Worse?
Crohn’s disease is progressive in structure even when it is intermittent in symptoms. The Montreal classification describes disease behaviour in three categories: B1, inflammatory disease without stricture or fistula; B2, stricturing disease; and B3, penetrating disease with fistula or abscess. At diagnosis the large majority of patients are B1. Within twenty years, roughly half have progressed to B2 or B3.
That progression is the natural history of untreated or undertreated transmural inflammation. Each flare deposits a little more collagen. The bowel wall thickens, the lumen narrows, and at some point the narrowing stops being reversible. Symptoms may fluctuate and can settle completely between flares, but the structural damage only accumulates. Inflammation can go to zero. Fibrosis only goes up.
This asymmetry is the reason the timing of a transplant decision matters as much as the decision itself. A patient in the inflammatory phase, with active disease and little accumulated fibrosis, is a patient whose immune system is doing the damage right now and can therefore be helped by resetting it. A patient who has already accumulated multiple fibrotic strictures over two decades has a mechanical problem that an immune reset does not address, whatever their symptom score says.
What Are the Stages of Crohn’s Disease?
Crohn’s disease is not staged in the way a cancer is staged. It is classified, and the classification that matters for a treatment decision is the Montreal classification, which describes three axes: age at diagnosis, location of disease, and behaviour. Behaviour is the axis that determines whether transplantation can help.
The behaviour categories describe what the inflammation has already done to the bowel. They are not a severity scale and a patient can move between them in only one direction.
| Montreal behaviour | What it means | Can HSCT help? |
|---|---|---|
| B1 Inflammatory | Active inflammation, no stricture and no fistula. The bowel wall is inflamed but not yet scarred. | Yes. This is the pattern in which the published remission rates were achieved. |
| B2 Stricturing | Fibrotic narrowing of the bowel. Scar tissue laid down by past inflammation. | Only the inflammatory component. A fixed fibrotic stricture will not open. |
| B3 Penetrating | Fistula or abscess. Inflammation has burrowed through the full thickness of the wall. | Limited. Any abscess must be drained and any sepsis treated before transplantation is safe. |
Table 1. Montreal classification of Crohn’s disease behaviour, and what each pattern means for transplantation. Behaviour progresses in one direction only.
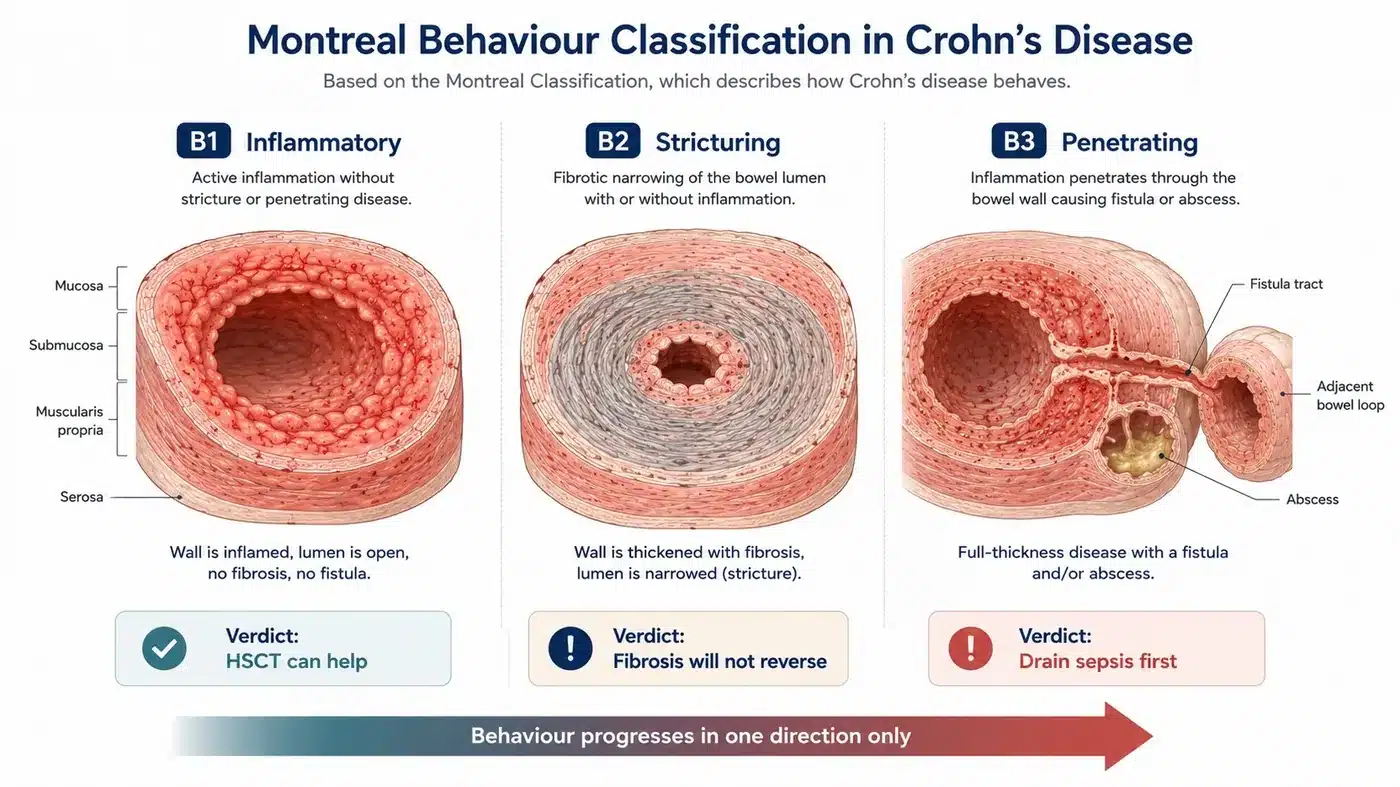
Figure 5. Montreal behaviour patterns. Inflammation can go to zero. Fibrosis only goes up.
Is Crohn’s Disease the Same as Ulcerative Colitis?
Crohn’s disease and ulcerative colitis are both inflammatory bowel diseases but they are different conditions and they respond differently to transplantation. Ulcerative colitis is confined to the colon, involves only the innermost lining of the bowel, and is continuous from the rectum upward. Crohn’s disease can occur anywhere in the digestive tract, is transmural, and is patchy.
The practical consequence is surgical. Because ulcerative colitis is confined to the mucosa of the colon, removing the colon removes the disease, and colectomy is genuinely curative. Crohn’s disease has no such operation. Resecting a diseased segment relieves the obstruction but the disease recurs, characteristically at the site of the join, in a majority of patients within a decade. This is the central difference and it is why the search for a durable immunological treatment in Crohn’s disease has been so much more urgent than in ulcerative colitis.
Because Crohn’s disease is transmural, it also produces the complications that ulcerative colitis does not: fistulas, abscesses and fibrotic strictures. Those complications are what turn a medical problem into a surgical one, and they are what a transplant, acting only on inflammation, cannot undo once established.
What Happens If Crohn’s Disease Goes Untreated?
Untreated Crohn’s disease progresses to structural bowel damage, and the consequences are cumulative and largely irreversible. The sequence is consistent: sustained transmural inflammation leads to fibrosis, fibrosis leads to stricture, stricture leads to obstruction, and obstruction leads to surgery. Around half of patients with Crohn’s disease require intestinal resection within ten years of diagnosis.
Repeated resection carries its own price. Each operation removes a length of small bowel, and enough resections produce short bowel syndrome, in which the remaining intestine cannot absorb sufficient nutrition and the patient becomes dependent on intravenous feeding. Penetrating disease produces fistulas and intra-abdominal abscesses, which can require emergency surgery and a temporary or permanent stoma.
There are further consequences beyond the bowel. Long-standing Crohn’s colitis raises the risk of colorectal cancer. Chronic inflammation and repeated corticosteroid courses cause osteoporosis. Iron and vitamin B12 deficiency follow from bleeding and from loss of the terminal ileum where B12 is absorbed. Growth failure in children with Crohn’s disease is common and is not fully recoverable once puberty has passed.
Every one of these outcomes began as inflammation and ended as damage. That is the argument for intervening while the disease is still an immunological problem rather than a structural one.
How Is Crohn’s Disease Usually Treated Before HSCT Is Considered?
Conventional treatment for Crohn’s disease escalates through corticosteroids, immunomodulators and biologic drugs, with surgery reserved for complications. This escalation is set out in the NICE guideline on Crohn’s disease management (NG129) and in the European Crohn’s and Colitis Organisation guidelines, and a transplant is considered only once that ladder has been exhausted. Corticosteroids such as prednisolone and budesonide induce remission quickly but do not maintain it, and their long-term use causes osteoporosis, diabetes, cataract and adrenal suppression. They are a bridge, not a treatment.
Immunomodulators, principally azathioprine and methotrexate, maintain remission in some patients and are often used alongside a biologic to reduce the formation of antibodies against it. Biologic drugs are the mainstay of modern maintenance therapy and fall into distinct classes: anti-TNF agents such as infliximab and adalimumab, the anti-integrin vedolizumab, and the anti-interleukin agents ustekinumab and risankizumab. The small molecule JAK inhibitor upadacitinib is the most recent addition.
Surgery is not a failure of medical treatment and it is often the correct answer. An ileocaecal resection for a short, fixed, fibrotic stricture in a patient without significant inflammation elsewhere is a good operation with a good outcome. The problem is not surgery. The problem is that surgery treats the fibrosis and leaves the immune disease intact, and so the disease returns above the anastomosis.
Before any patient is considered refractory, one question must be answered: were the drugs actually failing, or were they never properly delivered? Therapeutic drug monitoring measures the concentration of a biologic in the blood and the presence of antibodies against it. A significant proportion of patients labelled as having failed a biologic are found on testing to have had a sub-therapeutic drug level or to have developed anti-drug antibodies, both of which are correctable by dose escalation or by adding an immunomodulator. A patient in that position does not need a transplant. They need their dose adjusted. We test for this before we discuss transplantation, and it is one of the reasons some patients referred to us are sent back to their gastroenterologist rather than to a transplant ward.
 Get HSCT India Brochure Emailed to you
Get HSCT India Brochure Emailed to you
Can HSCT Treat Crohn’s Disease? What the Evidence Shows
Autologous haematopoietic stem cell transplantation produces clinical remission in approximately 79 percent and endoscopic remission in approximately 82 percent of patients with refractory Crohn’s disease across the published series, according to a systematic review and meta-analysis of the pooled data (PubMed 28658168). In the Northwestern series led by Professor Richard K. Burt, eleven of twelve patients with treatment-refractory disease entered sustained clinical remission (PubMed 12393477). In a subsequent non-myeloablative series, the mean Crohn’s Disease Activity Index fell from 281 before transplant to 96 at thirty days, with low toxicity and a measurable improvement in quality of life (PubMed 28985769). The non-myeloablative protocol pioneered by Professor Burt is the same protocol we use in HSCT for multiple sclerosis, where the evidence base is largest, and it is the protocol used at HSCT Hospital India.
These results come from patients who had exhausted conventional therapy. They had failed corticosteroids, failed immunomodulators, and failed one or more classes of biologic drug. Many had already had surgery. They were not patients with mild disease who might have done well on any treatment. They were patients for whom no further medical option existed.
Two randomised controlled trials have tested HSCT in Crohn’s disease, and neither met its primary endpoint. The ASTIC trial used a deliberately stringent composite endpoint requiring steroid-free clinical remission for three months with no endoscopic or radiological evidence of inflammation, and few patients achieved it. Measured against the endpoints conventionally used in Crohn’s drug trials, the same data showed clinical remission in 44 percent of transplanted patients versus 9 percent of controls at one year, and regression of all endoscopic ulceration in half of those transplanted, but the trial carried a high burden of serious adverse events including one death (PubMed 28497755). ASTIClite, which tested a reduced-intensity conditioning regimen intended to be safer, was stopped early after twenty-three patients on the advice of its data monitoring committee following a high incidence of serious adverse events and one patient death (PubMed 38408175). Pooled transplant-related mortality across the Crohn’s series is approximately 6.4 percent, which is substantially higher than the figure reported for multiple sclerosis. Any centre that presents HSCT for Crohn’s disease as a routine or low-risk procedure is misrepresenting the evidence, and a patient should treat that presentation as a warning about the centre.
The gap between the observational results and the randomised results is explained by the distinction this guide has followed from the first section. HSCT acts on inflammation. It does not act on fibrosis. Both randomised trials recruited patients with long-standing refractory disease, and long-standing refractory disease carries accumulated fibrotic and structural damage that no immune reset can reverse. Patient selection is therefore not a preliminary to the treatment. Patient selection is the treatment decision. The patient with active inflammatory disease, a raised faecal calprotectin, endoscopic ulceration and a low burden of fibrosis is the patient in whom the published remission rates were achieved. Establishing whether you are that patient is precisely what a formal transplant evaluation exists to determine, and it is the reason we decline to transplant a substantial proportion of the patients who ask us to.
| Study | Design | Outcome | Safety |
|---|---|---|---|
| Pooled meta-analysis | Systematic review of published series | 79% clinical remission; 82% endoscopic remission | Transplant-related mortality approx 6.4% |
| Burt, Northwestern (2003) | Case series, refractory disease | 11 of 12 patients in sustained clinical remission | Low toxicity on the non-myeloablative regimen |
| Ruiz, non-myeloablative (2017) | Case series, 14 patients | Mean CDAI 281 before transplant, 96 at day 30 | Low toxicity; quality of life improved |
| ASTIC (2017) | Randomised controlled trial | Primary endpoint not met. By conventional endpoints: 44% vs 9% clinical remission at 1 year; all ulceration cleared in 50% | High adverse event burden; one death |
| ASTIClite (2024) | Randomised controlled trial, reduced intensity | Stopped early after 23 patients | Serious adverse events; one patient death |
| EBMT long-term survey (2018) | Retrospective, long-term follow-up | Durable benefit in a proportion; relapse rises with time | Confirms the toxicity signal |
Table 2. The evidence for HSCT in Crohn’s disease, positive and negative. Both randomised trials failed their primary endpoints. Patient selection explains most of the gap.
How Does a Stem Cell Transplant for Crohn’s Disease Work?
Autologous HSCT for Crohn’s disease works by removing the misdirected immune system and rebuilding a new one from the patient’s own haematopoietic stem cells. Autologous means the cells come from the patient, so there is no donor, no tissue matching and no risk of graft-versus-host disease, the condition in which donated immune cells attack the recipient. The lymphocytes that have learned to attack the bowel wall are eliminated, and the stem cells that are reinfused have not learned that behaviour. The immune system that regrows is naive.
The procedure has four stages and they are always performed in this order.
Mobilisation. The patient receives cyclophosphamide followed by granulocyte colony stimulating factor, or G-CSF. This drives haematopoietic stem cells out of the bone marrow and into the circulating blood, where they can be collected.
Harvest (Leukapheresis). Blood is drawn through a cell separator, which removes the CD34-positive stem cells and returns everything else to the patient. The graft is then cryopreserved, meaning frozen and stored, while the next stage is carried out. The procedure takes a few hours and does not require anaesthesia.
Conditioning. This is the immunoablative stage, in which the existing immune system is destroyed. We use a non-myeloablative regimen, meaning the dose is calibrated to ablate the immune system without permanently destroying the bone marrow itself. The regimen is based on cyclophosphamide with anti-thymocyte globulin, which is an antibody preparation that specifically depletes T lymphocytes. The distinction from a myeloablative regimen is not a marketing point. It is the reason transplant-related mortality in this protocol is lower than in the high-intensity regimens used in some earlier trials, and it is why we use it.
Reinfusion. The cryopreserved graft is thawed and returned to the patient through a central line. The stem cells find their way back to the bone marrow and begin producing blood cells again. The period between conditioning and engraftment is the aplastic phase, during which the patient has almost no white cells and is at genuine risk of infection. This phase is why the entire procedure is conducted as an inpatient in a Triple HEPA filtered isolation room and why it cannot responsibly be done as a day case.
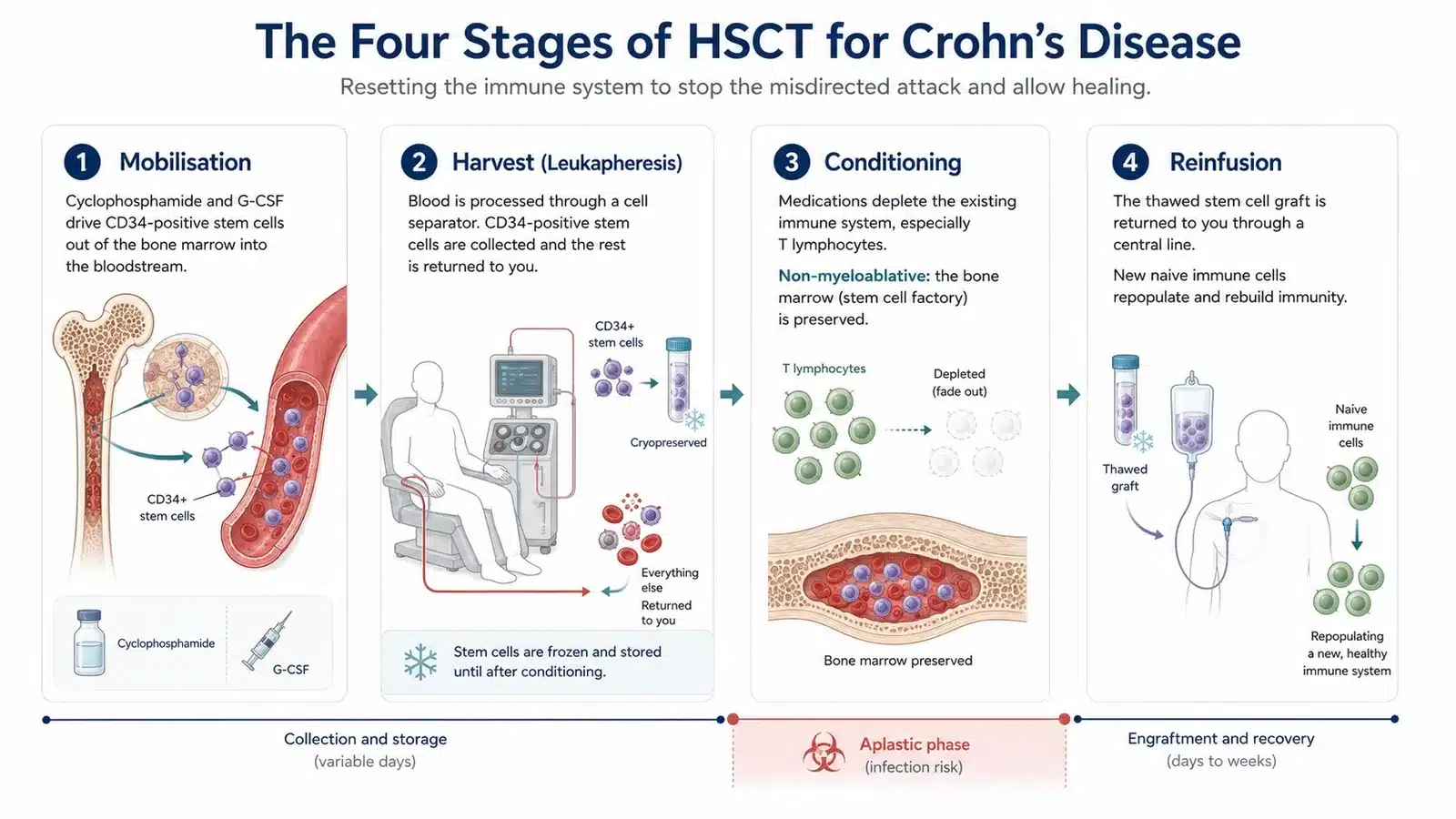
Figure 6. Autologous HSCT proceeds in four stages. The aplastic phase, the gap between conditioning and engraftment, carries the highest infection risk.
What Happens During the 30 Days in Hospital?
The HSCT programme at HSCT Hospital India runs for thirty days as an inpatient, and both the patient and one attendant are accommodated for the whole of that period. The schedule is deliberately unhurried because the aplastic phase cannot be rushed.
Days 1 to 5 are assessment and workup. Bloods, imaging, cardiac and pulmonary function testing, infection screening, and a colonoscopy or MRE if the outside imaging is not recent enough to establish the inflammation-to-fibrosis ratio. A central venous line is placed. If the assessment shows that the disease is predominantly fibrotic, the transplant does not proceed, and we say so at this point rather than after conditioning has begun.
Days 6 to 12 are mobilisation and harvest. Cyclophosphamide is given, followed by daily G-CSF. Stem cell counts are monitored and leukapheresis is performed when the CD34-positive count is adequate, usually over one or two sessions. The graft is cryopreserved.
Days 13 to 18 are conditioning. Cyclophosphamide and anti-thymocyte globulin are administered. Nausea, fatigue and hair loss begin in this window and are expected rather than a sign that something has gone wrong.
Day 19 is reinfusion. The graft is thawed at the bedside and returned intravenously. The infusion itself is uneventful and takes under an hour.
Days 20 to 30 are the aplastic phase and engraftment. This is the demanding part of the programme. The white cell count falls to near zero, and fever during this period is common and is treated immediately with broad spectrum antibiotics. The patient remains in the HEPA filtered room. Neutrophil engraftment, meaning the return of a working white cell count, typically occurs between ten and fourteen days after reinfusion, and discharge follows once engraftment is established and the patient is afebrile and eating.
There is no maintenance chemotherapy after discharge and no ongoing immunosuppression is planned. That is the point of the procedure. Immune reconstitution continues for twelve to twenty-four months after the patient goes home, and the clinical benefit is often still improving at one year.
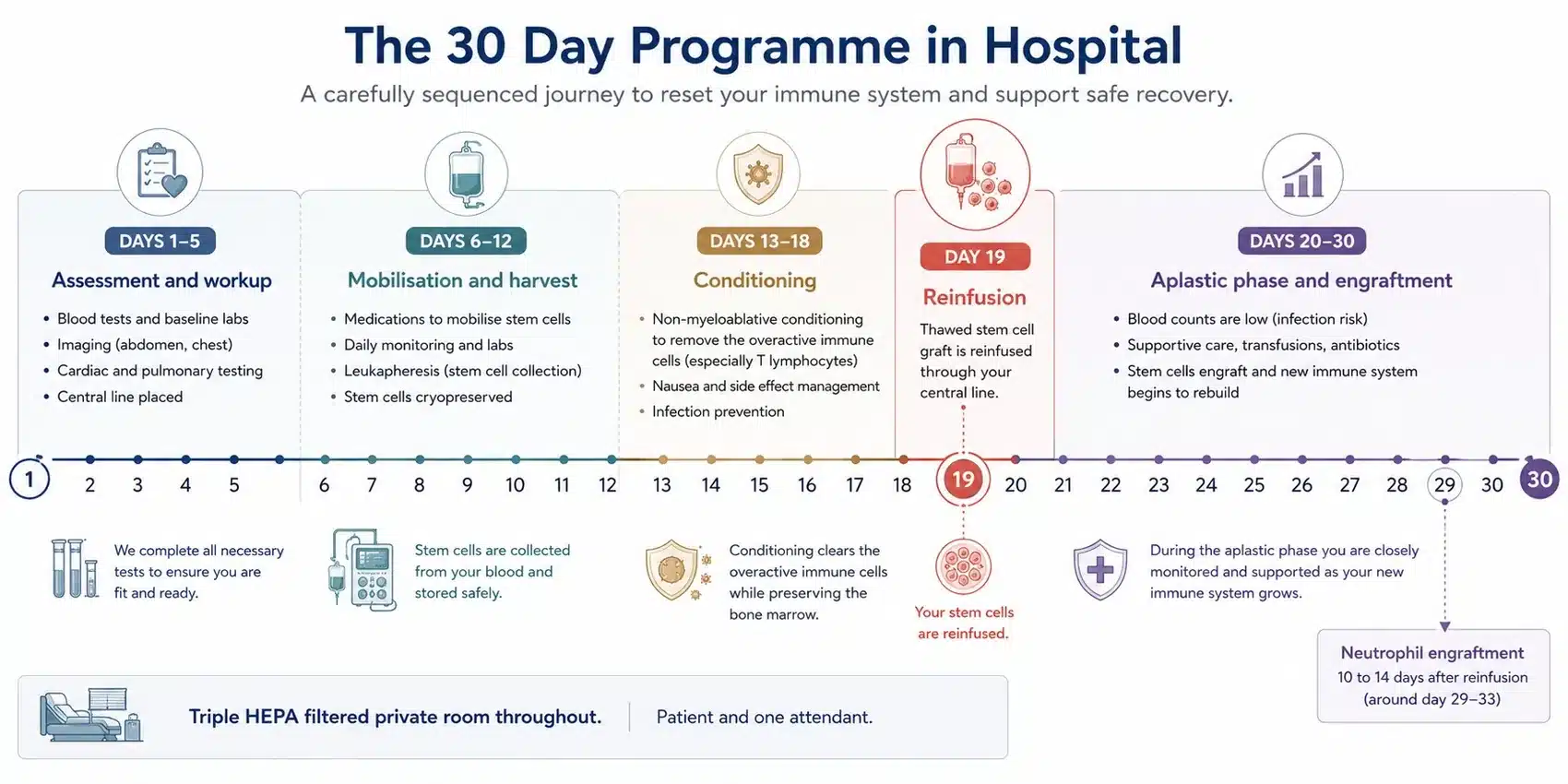
Figure 7. The 30 day inpatient programme. Patient and attendant are housed together for the entire admission.
The Risks of HSCT in Crohn’s Disease, and What We Do About Them
HSCT is a serious procedure with a real mortality risk, and in Crohn’s disease that risk is higher than in the conditions for which the procedure is better established. Pooled transplant-related mortality across the published Crohn’s series is approximately 6.4 percent. The randomised ASTIClite trial was halted early after twenty-three patients because of serious adverse events including a death, and the earlier ASTIC trial also recorded a death. These are the facts, they are not disputed, and any patient considering this treatment is entitled to have them stated before they are asked to consider a cost.
The dominant risk is infection during the aplastic phase, the window between conditioning and engraftment when the patient has essentially no functioning immune system. Neutropenic sepsis is the principal cause of transplant-related death. It is managed by isolation in a Triple HEPA filtered room, prophylactic antimicrobials, daily monitoring and immediate empirical antibiotics at the first fever. The presence of a transplant infectious disease specialist on the team is not a decorative credential. It is the specialty most directly responsible for whether a patient survives this phase.
Expected effects of the conditioning regimen include nausea, mucositis, fatigue and alopecia, all of which resolve. Cyclophosphamide is gonadotoxic and can cause permanent infertility. Fertility preservation, meaning sperm banking or oocyte or embryo cryopreservation, must be discussed and arranged before conditioning begins, and it cannot be arranged afterwards. Late effects include a small increase in the risk of secondary malignancy and of autoimmune thyroid disease.
The risk is not evenly distributed. It concentrates in patients who are malnourished, who have active sepsis or an undrained abscess, who have significant comorbidity, or who have a heavy burden of fibrotic disease that the transplant cannot help anyway. Those patients carry the risk of the procedure without the prospect of the benefit, which is why they are not offered it. The single most effective thing a transplant centre does to reduce transplant-related mortality is to decline the patients who should not be transplanted.
Should I Choose HSCT or CAR T Cell Therapy for Crohn’s Disease?
CAR T cell therapy is not an established treatment for Crohn’s disease and should not currently be considered an alternative to HSCT. Chimeric antigen receptor T cell therapy, in which a patient’s T cells are genetically engineered to target a specific antigen, has produced striking results in refractory lupus and in some other antibody-driven autoimmune conditions, where it works by eliminating the B cells that produce autoantibodies. The comparison between transplantation and CAR T cell therapy is set out in full on our lupus stem cell therapy guide.
Crohn’s disease is not primarily an autoantibody-driven disease. It is driven by a T cell mediated response to gut bacteria, and the B cell depletion that makes CAR T therapy effective in lupus does not have the same rationale here. Only a small number of patients with inflammatory bowel disease have received CAR T cell therapy anywhere in the world, in early-phase research settings, and there is no published trial evidence supporting its routine use.
For a patient with refractory Crohn’s disease today, the practical position is that HSCT has decades of published outcome data including two randomised trials, and CAR T therapy does not. That is a statement about the current evidence and not a prediction. If a patient is offered CAR T cell therapy for Crohn’s disease outside a registered clinical trial, they should ask to see the published data supporting it.
| HSCT | CAR T cell therapy | |
|---|---|---|
| Mechanism | Removes and rebuilds the whole immune system from your own stem cells | Engineers T cells to deplete a specific target, usually B cells |
| Rationale in Crohn’s | Directly addresses the T cell response to gut bacteria that drives the disease | Depletes autoantibody-producing B cells, which is not the main driver in Crohn’s |
| Evidence in Crohn’s | Decades of published series plus two randomised trials | No published trial evidence. Only a small number of IBD patients treated anywhere |
| Availability | Established programme, including at HSCT Hospital India | Early-phase research settings only |
Table 3. HSCT compared with CAR T cell therapy for Crohn’s disease.
Can Crohn’s Disease Be Cured?
Autologous HSCT is the only treatment for Crohn’s disease that has been shown to produce sustained, drug-free remission after a single course, and in the published series a majority of carefully selected refractory patients achieve clinical and endoscopic remission. Patients who have depended on biologic infusions for years frequently leave the programme on no Crohn’s medication at all.
No treatment for Crohn’s disease is described in the medical literature as a cure, and any centre that uses the word should be treated with caution. The genetic susceptibility that underlies the disease is not altered by a transplant, and neither is the gut microbiome that the immune system reacts against. What changes is the immune response that sits between them.
A proportion of patients relapse. In the published long-term follow-up, relapse rates rise with time from transplant, and some patients resume medication. There is an important observation in that group: biologic drugs that had stopped working before the transplant frequently begin working again afterwards. A patient who had failed infliximab and adalimumab and had no medical options left can find, after immune reconstitution, that they respond to a drug that had failed them. Regaining a treatment option is itself a clinically meaningful outcome, and it is one that is rarely explained to patients before they decide.
 Request a Call Back
Request a Call BackWho Qualifies for a Crohn’s Transplant, and How We Assess It
You are a candidate for HSCT if your Crohn’s disease is active, inflammatory and refractory to conventional therapy, and if you have not yet accumulated a heavy burden of fibrotic damage. That single sentence is the conclusion of everything above, and it is worth restating in the terms a transplant team actually uses.
Active and inflammatory means there is objective evidence of ongoing inflammation now, not merely symptoms. That means endoscopic ulceration, a raised faecal calprotectin, and inflammatory change on MRE or intestinal ultrasound. A patient with obstructive symptoms, a normal calprotectin and a fixed fibrotic stricture on imaging has a mechanical problem. They are referred to a surgeon, and a transplant would expose them to a 6.4 percent mortality risk in exchange for nothing.
Refractory means the conventional options have genuinely been exhausted, not merely tried. Before we accept that a biologic has failed, we look for a measured drug level and an antibody titre. A patient with a sub-therapeutic infliximab level has not failed infliximab. They have been underdosed, and the correct next step is dose escalation, not transplantation. There is no internationally agreed definition of refractory Crohn’s disease, which is why different centres give different patients different answers, and it is why we set out our own threshold explicitly rather than leaving the patient to guess at it.
Fitness for the procedure is assessed separately: cardiac and pulmonary function, renal function, nutritional status, absence of active untreated infection or undrained abscess, and absence of malignancy. Age is not an absolute barrier but physiological reserve is. Fertility preservation is discussed before conditioning, never after.
The patients who benefit most are those with active inflammatory disease of the Montreal B1 pattern who have failed two or more classes of biologic, who have a low fibrotic burden, who are nutritionally adequate, and who have no untreated sepsis. The patients who should not be transplanted are those with predominantly fibrostenotic or penetrating disease, active untreated infection, significant organ dysfunction, or malnutrition that has not been corrected. We say no to a substantial proportion of the patients who ask us, and that is not a limitation of the programme. It is the programme.
Crohn’s Disease HSCT Cost in India, and the Global Picture
HSCT at HSCT Hospital India costs 30,000 US dollars as an all-inclusive HSCT treatment package, covering thirty days as an inpatient for the patient and one attendant. The same procedure in the United States is generally quoted at between 150,000 and 200,000 US dollars, and is in most cases not funded by insurance for Crohn’s disease because the procedure is regarded as investigational.
The package includes the full thirty day hospital stay in a deluxe private room with Triple HEPA triple-level air filtration, all doctors’ fees, all consultations, all investigations and laboratory tests, all medicines and consumables, the mobilisation, the leukapheresis, the cryopreservation, the conditioning regimen, the reinfusion, nursing care, physiotherapy, food and laundry for both the patient and the attendant, and airport transfers. There are no hidden charges and no separate itemised billing at discharge.
The comparison that most patients have not made is with the cost of continuing conventional therapy. A patient maintained on a biologic drug indefinitely incurs a recurring annual cost for the rest of their life, and that cost continues whether or not the drug is still working. The relevant comparison for a refractory patient is not the transplant against nothing. It is the transplant against another two decades of escalating therapy, repeated hospital admissions and, in around half of patients, intestinal surgery.
| Country | Typical cost (USD) | Notes |
|---|---|---|
| India (HSCT Hospital India) | $30,000 | All-inclusive. 30 days inpatient, patient plus attendant, deluxe private room with Triple HEPA filtration. No hidden charges. |
| United States | $150,000 to $200,000 | For Crohn’s disease this is usually treated as investigational, so insurers rarely fund it. |
| Continuing biologic therapy | Recurring, indefinite | The relevant comparison for a refractory patient is not the transplant against nothing. It is the transplant against decades of escalating therapy and, in around half of patients, intestinal surgery. |
Table 4. What HSCT for Crohn’s disease costs, country by country.
Frequently Asked Questions About Crohn’s Disease New Treatment
Is HSCT a new treatment for Crohn’s disease?
HSCT is not new as a procedure. It has been used in haematology for decades and has been studied in Crohn’s disease since the early 2000s. What is relatively new is its use in carefully selected refractory patients using a non-myeloablative conditioning regimen, which is calibrated to reset the immune system without permanently destroying the bone marrow, and which carries a lower risk than the high-intensity regimens used in earlier work.
What is the success rate of stem cell transplant for Crohn’s disease?
Across the published series, autologous HSCT produces clinical remission in approximately 79 percent and endoscopic remission in approximately 82 percent of patients with refractory Crohn’s disease. These figures come from carefully selected patients with active inflammatory disease. Two randomised controlled trials did not meet their primary endpoints, and patient selection is the main factor that explains the difference.
Is HSCT for Crohn’s disease dangerous?
HSCT carries a real risk of death. Pooled transplant-related mortality across the published Crohn’s disease series is approximately 6.4 percent, and one randomised trial, ASTIClite, was stopped early after twenty-three patients because of serious adverse events including a patient death. The principal danger is infection during the aplastic phase, the period after conditioning when the patient has almost no immune system. It is managed with isolation in a Triple HEPA filtered room and immediate treatment of any fever.
Can HSCT cure Crohn’s disease?
No treatment for Crohn’s disease is described in the medical literature as a cure, and a centre that promises one should be treated with caution. HSCT is the only treatment shown to produce sustained drug-free remission after a single course. A proportion of patients relapse, and among those who do, biologic drugs that had stopped working before the transplant frequently start working again afterwards.
Will HSCT fix my strictures?
No. HSCT acts on inflammation, not on fibrosis. A fibrotic stricture is scar tissue laid down by past inflammation, and no drug and no transplant dissolves it. A narrowed segment that is inflamed rather than scarred can improve. Distinguishing the two requires magnetic resonance enterography or intestinal ultrasound, and it is the first thing we establish, because a patient whose disease is predominantly fibrotic needs a surgeon rather than a transplant.
Who is not eligible for HSCT for Crohn’s disease?
Patients with predominantly fibrostenotic disease, active untreated infection or an undrained abscess, significant cardiac, pulmonary or renal dysfunction, uncorrected malnutrition, or malignancy are not offered transplantation. Patients labelled refractory who are found on testing to have a sub-therapeutic biologic drug level or anti-drug antibodies are also not transplanted, because their drug can usually be made to work with a dose adjustment.
How long does recovery from HSCT take?
The inpatient programme is thirty days. Neutrophil engraftment usually occurs ten to fourteen days after reinfusion. Fatigue commonly persists for three to six months after discharge. Immune reconstitution continues for twelve to twenty-four months, and clinical improvement is often still continuing at one year. There is no maintenance chemotherapy after discharge.
Does HSCT affect fertility?
Cyclophosphamide, which is used in both mobilisation and conditioning, is gonadotoxic and can cause permanent infertility. Fertility preservation, meaning sperm banking or oocyte or embryo cryopreservation, must be arranged before conditioning begins. It cannot be arranged afterwards, and it is discussed with every patient of reproductive age as part of the assessment.
How much does HSCT for Crohn’s disease cost in India?
HSCT at HSCT Hospital India is an all-inclusive package of 30,000 US dollars, covering thirty days as an inpatient for the patient and one attendant, in a deluxe private room with Triple HEPA filtration. The same procedure costs between 150,000 and 200,000 US dollars in the United States, where it is generally not funded by insurance for Crohn’s disease.
Is CAR T cell therapy better than HSCT for Crohn’s disease?
CAR T cell therapy is not an established treatment for Crohn’s disease. It works by depleting the B cells that produce autoantibodies, which is why it has shown promise in lupus. Crohn’s disease is driven primarily by a T cell response to gut bacteria rather than by autoantibodies, so the rationale does not transfer. Only a small number of patients with inflammatory bowel disease have received it anywhere, in early-phase research settings.
What Is the Next Step?
Nothing in this guide can tell you whether HSCT is the right treatment for you. That question is answered by a formal transplant evaluation, which reviews your endoscopy, your cross-sectional imaging, your faecal calprotectin, your biologic drug levels and your organ reserve together, and which establishes the one thing that decides the outcome: how much of your disease is inflammation that can be reset, and how much is fibrosis that cannot.
That evaluation is exactly what we provide. We turn down a sizeable share of the people who approach us, and we say so before anyone travels rather than after. The sections below introduce the centre where the evaluation is carried out.
People who have already completed the programme have set down their own accounts of it. Click here to watch patient testimonial videos.
Click here to request a free HSCT eligibility assessment
Why Choose HSCT Hospital India for Life Changing Crohn’s Disease Treatment

 Complete 30 day HSCT done in hospital. Private deluxe rooms are very well served for patient and attendant comfort and equipped with HEPA Filter with Triple Level Air Filtration. No outside hospital stay avoids risk of infection during the aplastic phase, 24 x 7 nursing care and best medical attention. Advanced HSCT protocol used does not require any further chemo or treatment after leaving the hospital. Click here to get complete details
Complete 30 day HSCT done in hospital. Private deluxe rooms are very well served for patient and attendant comfort and equipped with HEPA Filter with Triple Level Air Filtration. No outside hospital stay avoids risk of infection during the aplastic phase, 24 x 7 nursing care and best medical attention. Advanced HSCT protocol used does not require any further chemo or treatment after leaving the hospital. Click here to get complete details
 International and Globally Renowned Accreditations. HSCT Hospital India is accredited by the Joint Commission International, USA, the National Accreditation Board for Hospitals and Healthcare Providers (NABH), and the National Accreditation Board for Laboratories (NABL) for processes and high quality patient care. The non-myeloablative protocol pioneered by Professor Richard K. Burt is the protocol used here. Click here to know more
International and Globally Renowned Accreditations. HSCT Hospital India is accredited by the Joint Commission International, USA, the National Accreditation Board for Hospitals and Healthcare Providers (NABH), and the National Accreditation Board for Laboratories (NABL) for processes and high quality patient care. The non-myeloablative protocol pioneered by Professor Richard K. Burt is the protocol used here. Click here to know more

Real Patient– Real Stories


