HSCT for Multiple Sclerosis (MS): Life Changing Stem Cell Treatment
Medically reviewed by Dr. Rahul Bhargava, MBBS, MD (Medicine), DM (Clinical Haematology, AIIMS), Fellowship in Stem Cell Transplantation, Vancouver. Principal Director and Chief of HSCT, Haematology, Haemato-Oncology and Bone Marrow Transplantation, HSCT Hospital India.
Last reviewed: 16 July 2026. This guide cites peer-reviewed studies, which are linked throughout.
This guide explains when HSCT should be considered, what the evidence shows, who is eligible, what the treatment involves day by day, and what to realistically expect. It is written for people with active, relapsing MS who are weighing a transplant against staying on disease-modifying drugs. MS is the most studied of the conditions treated this way, and our overview of HSCT for autoimmune diseases sets out what the evidence shows across the rest of them.
What Is Multiple Sclerosis?
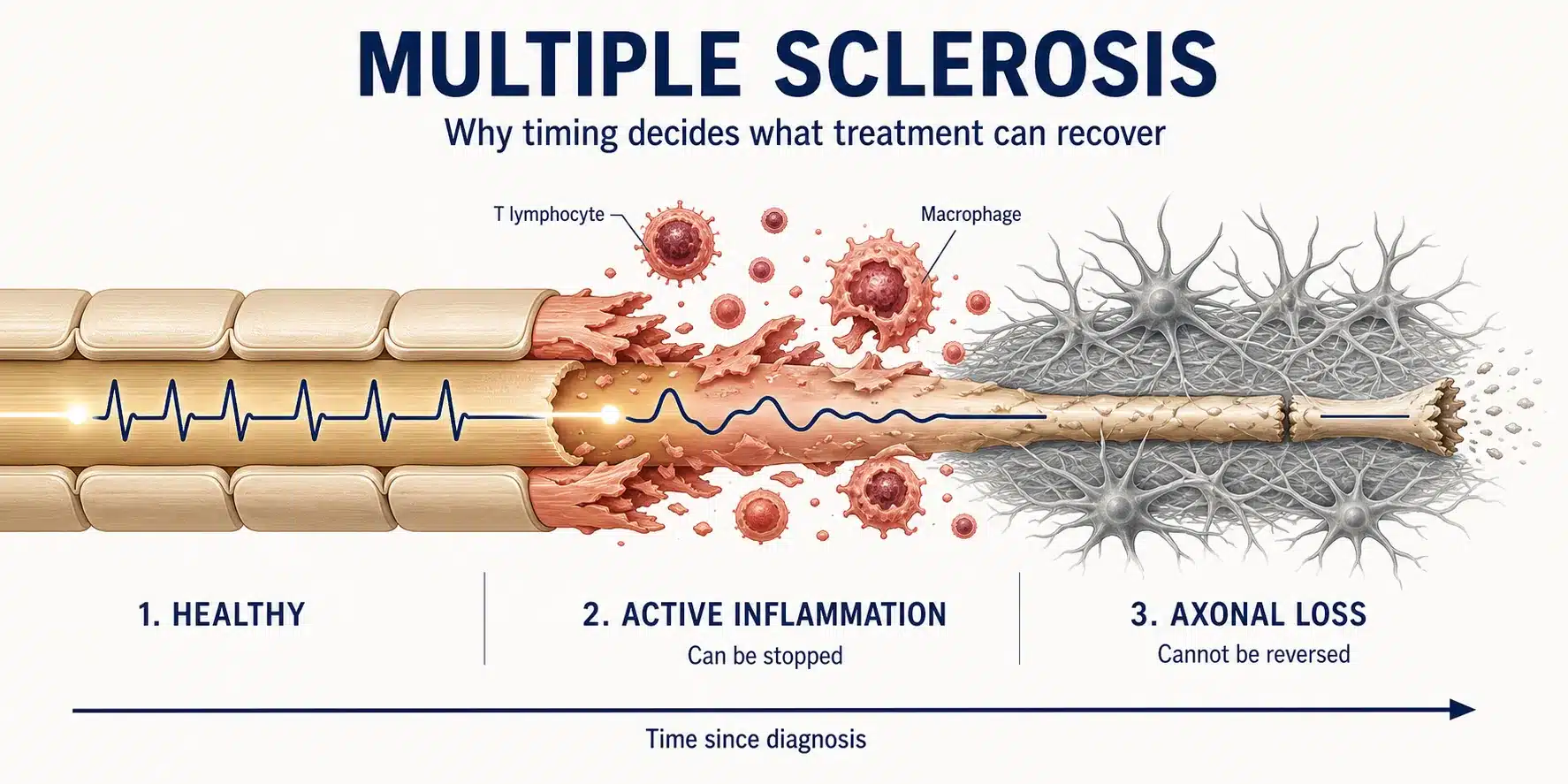
Multiple sclerosis is a disease in which the immune system attacks the myelin sheath, the fatty insulation around the nerve fibres of the brain, spinal cord and optic nerves. Where myelin is stripped away, the exposed nerve fibre conducts its signal slowly, or not at all, and eventually the fibre itself can be lost. That is the single fact that governs everything else on this page: MS has an inflammatory phase, in which the immune attack is active and reversible, and a degenerative phase, in which nerve fibres that have already been lost do not come back.
Autoantibodies and, more importantly in MS, autoreactive T and B lymphocytes cross into the central nervous system and drive this attack. The damage shows on an MRI scan as lesions, or plaques, scattered in space across the nervous system and accumulating over time. Roughly 2.9 million people live with MS worldwide, most diagnosed between the ages of twenty and forty, and it affects women about three times as often as men.
Understanding MS as two overlapping processes, inflammation now and degeneration later, is what allows a patient to understand why HSCT works spectacularly for some people and offers little for others. We return to this distinction in every section that follows.
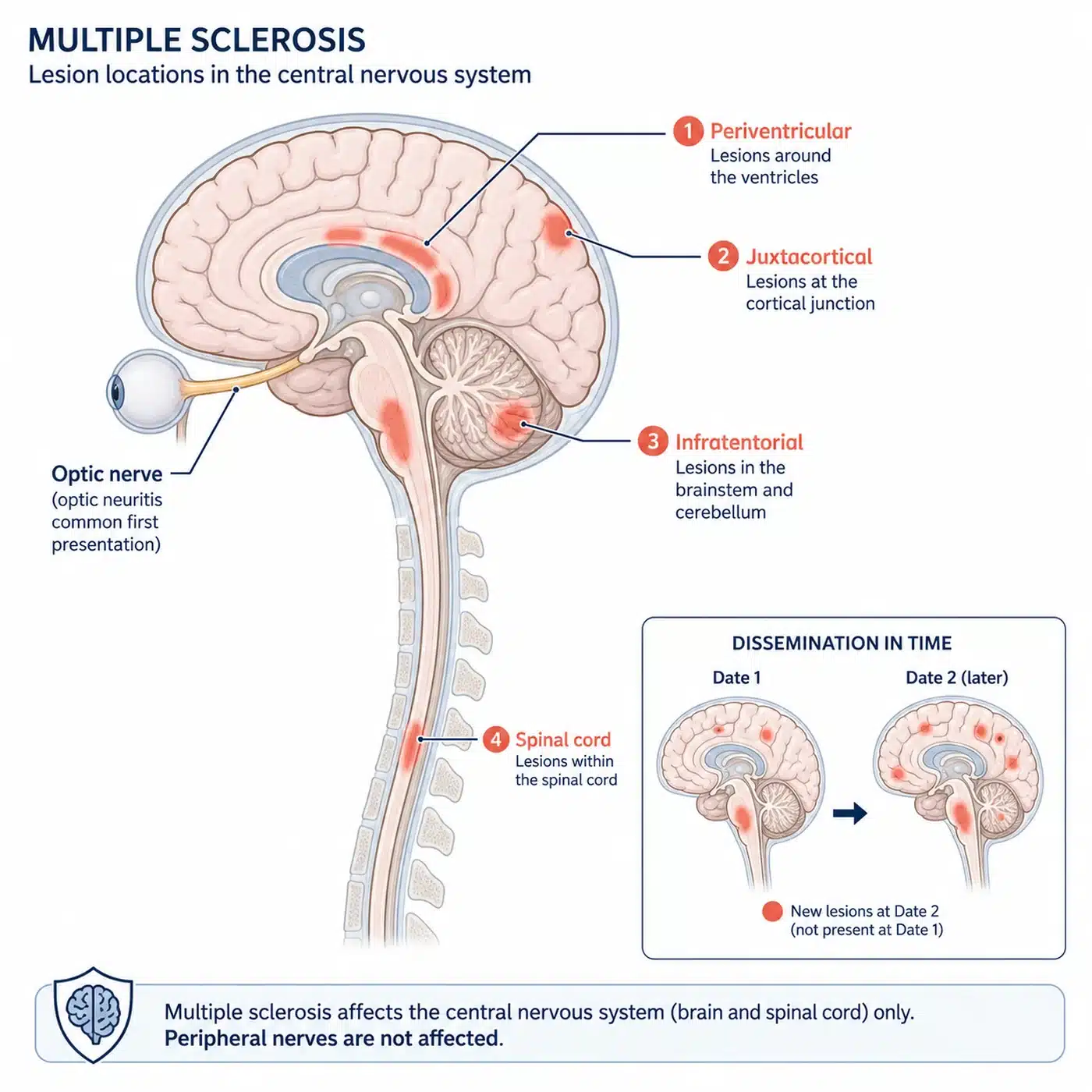
Figure 1. Multiple sclerosis damages the myelin at scattered sites across the brain, spinal cord and optic nerves. These lesions, disseminated in space and time, are what the diagnosis looks for.
MS Symptoms: How Demyelination Shows Up, Relapse to Relapse
Because MS lesions can appear anywhere in the central nervous system, its symptoms are unusually varied. The most common first symptoms are optic neuritis, which is pain and loss of vision in one eye, and sensory disturbance, which is numbness, tingling or a band-like tightness in a limb or around the trunk. As the disease continues, patients commonly develop:
- Fatigue that is out of all proportion to activity, the single most disabling symptom for many people
- Weakness and spasticity in the legs, causing difficulty walking
- Loss of balance and coordination
- Bladder urgency and bowel disturbance
- Cognitive fog, affecting memory, attention and processing speed
- Neuropathic pain and Lhermitte’s sign, an electric-shock sensation on bending the neck
- Heat sensitivity, in which symptoms worsen transiently when body temperature rises
A relapse, also called a flare or exacerbation, is the appearance of a new symptom or the clear worsening of an old one, lasting more than twenty-four hours and separated from the last relapse by at least a month. Each relapse reflects a new patch of active inflammation. Some relapses resolve completely. Others leave a permanent deficit behind, and that residue is the accumulated damage that a transplant cannot later reverse.
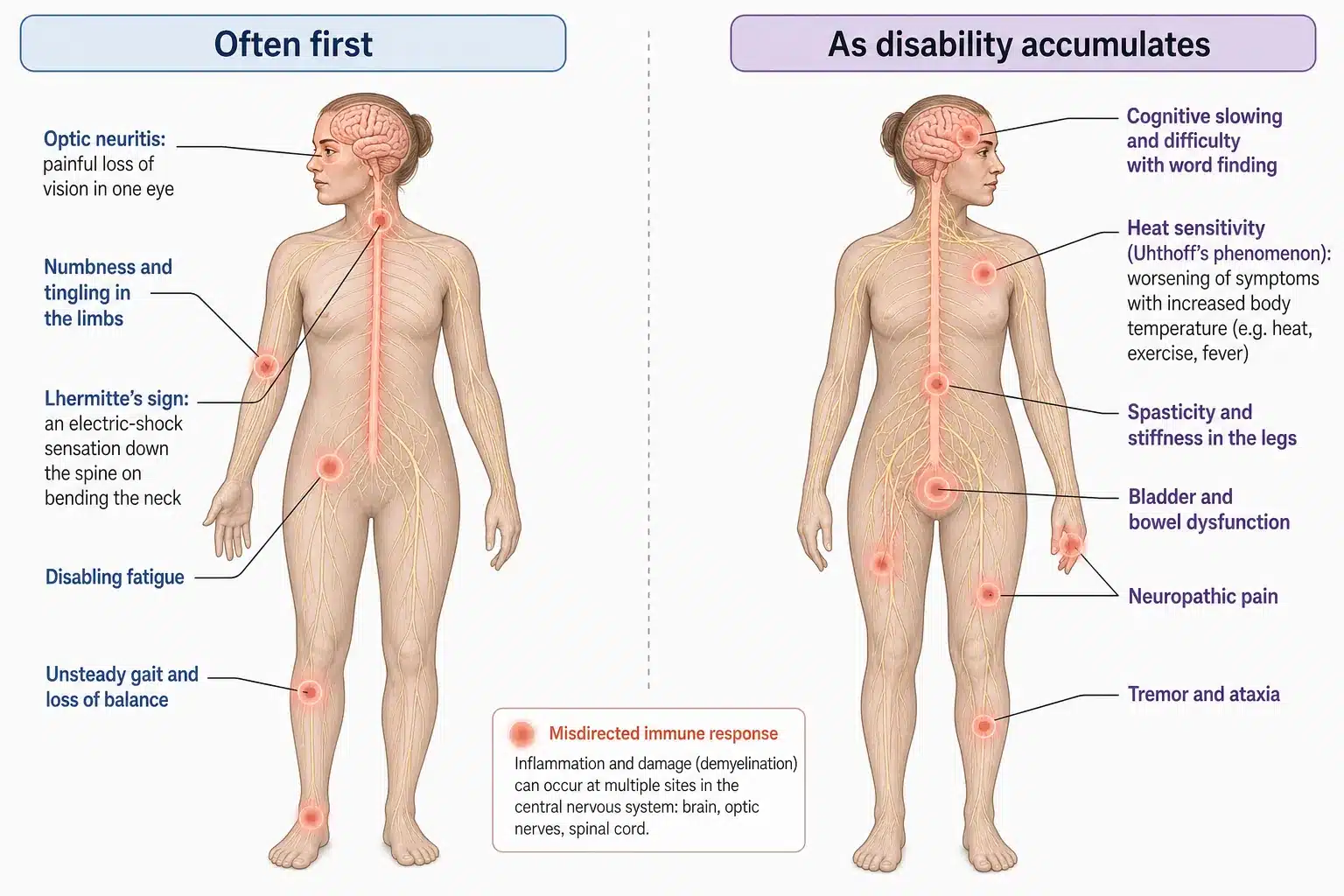
Figure 2. MS symptoms range from optic neuritis and numbness at first presentation to spasticity, bladder dysfunction and cognitive slowing as disability accumulates.
How Is MS Diagnosed?
MS is diagnosed using the McDonald criteria, which require evidence of damage disseminated in space, meaning lesions in more than one part of the central nervous system, and disseminated in time, meaning lesions that arose at different points. The tools are:
- MRI of the brain and spinal cord, with and without gadolinium contrast. A lesion that takes up contrast is actively inflamed and recent; a lesion that does not is older. This single distinction, the enhancing lesion, is the radiological signature of the inflammation that HSCT acts upon.
- Lumbar puncture, looking for oligoclonal bands, which are antibodies produced inside the central nervous system and found in the cerebrospinal fluid of the great majority of MS patients.
- Evoked potentials, which measure the speed of nerve conduction and can reveal damage the patient has not noticed.
The degree of disability is measured on the Expanded Disability Status Scale, or EDSS, which runs from 0, meaning no disability, to 10. A score up to 4.5 describes a patient who walks unaided; 6.0 means a walking aid is needed on one side; 7.0 and above means a wheelchair. The EDSS matters for eligibility, because HSCT works best while a patient is still in the inflammatory, relapsing phase and before disability has accumulated. You can read more about the scale in our guide to the EDSS score in multiple sclerosis.
What Triggers Multiple Sclerosis?
There is no single cause. MS arises where a genetic susceptibility meets an environmental trigger. The strongest single risk factor now known is prior infection with the Epstein-Barr virus, the virus that causes glandular fever; a large study of United States military recruits found that the risk of MS rose roughly thirty-two-fold after EBV infection, and almost every person who develops MS has been infected first. Low vitamin D and low sunlight exposure, which is why MS is commoner further from the equator, smoking, and adolescent obesity are the other established contributors. None of these is a reason for self-blame, and none can be undone, which is precisely why treatment focuses on the immune attack itself rather than its distant triggers.
Is MS Progressive? Will It Get Worse?
For most people MS begins as a relapsing-remitting disease, in which relapses are followed by periods of recovery and apparent stability. Left untreated, a substantial proportion of relapsing patients transition over ten to twenty years into secondary progressive MS, in which disability worsens steadily whether or not relapses continue. A minority, about one in ten, have primary progressive MS from the outset, with gradual decline and few or no distinct relapses.
The reason this matters is the activity-versus-damage distinction again. In the relapsing phase, the engine of disability is inflammation, and inflammation can be switched off. In the progressive phase, the engine is neurodegeneration, the slow loss of nerve fibres that were already injured, and that process does not respond to immune treatment. This is not a reason for despair: it is the reason to act while the disease is still inflammatory and still relapsing, when a transplant can change the entire trajectory.
What Are the Types of MS?
| Type | What it means | Response to HSCT |
|---|---|---|
| Relapsing-Remitting MS (RRMS) | Distinct relapses with partial or full recovery between them. The commonest form at diagnosis. | Best evidence. Active, relapsing RRMS is the group in which HSCT has been proven superior to drugs. |
| Secondary Progressive MS (SPMS), with active inflammation | Steady progression after an earlier relapsing course, but still with relapses or new MRI lesions. | Can benefit where inflammatory activity is still present. |
| Secondary Progressive MS, without activity | Steady progression with no relapses and no new lesions. | Limited benefit. The driver is degeneration, not inflammation. |
| Primary Progressive MS (PPMS) | Gradual decline from the start, without distinct relapses. | Generally not indicated, unless clear inflammatory activity is present. |
Table 1. The forms of multiple sclerosis and how each responds to HSCT. The single factor that predicts benefit is not the label but whether active inflammation is still present.
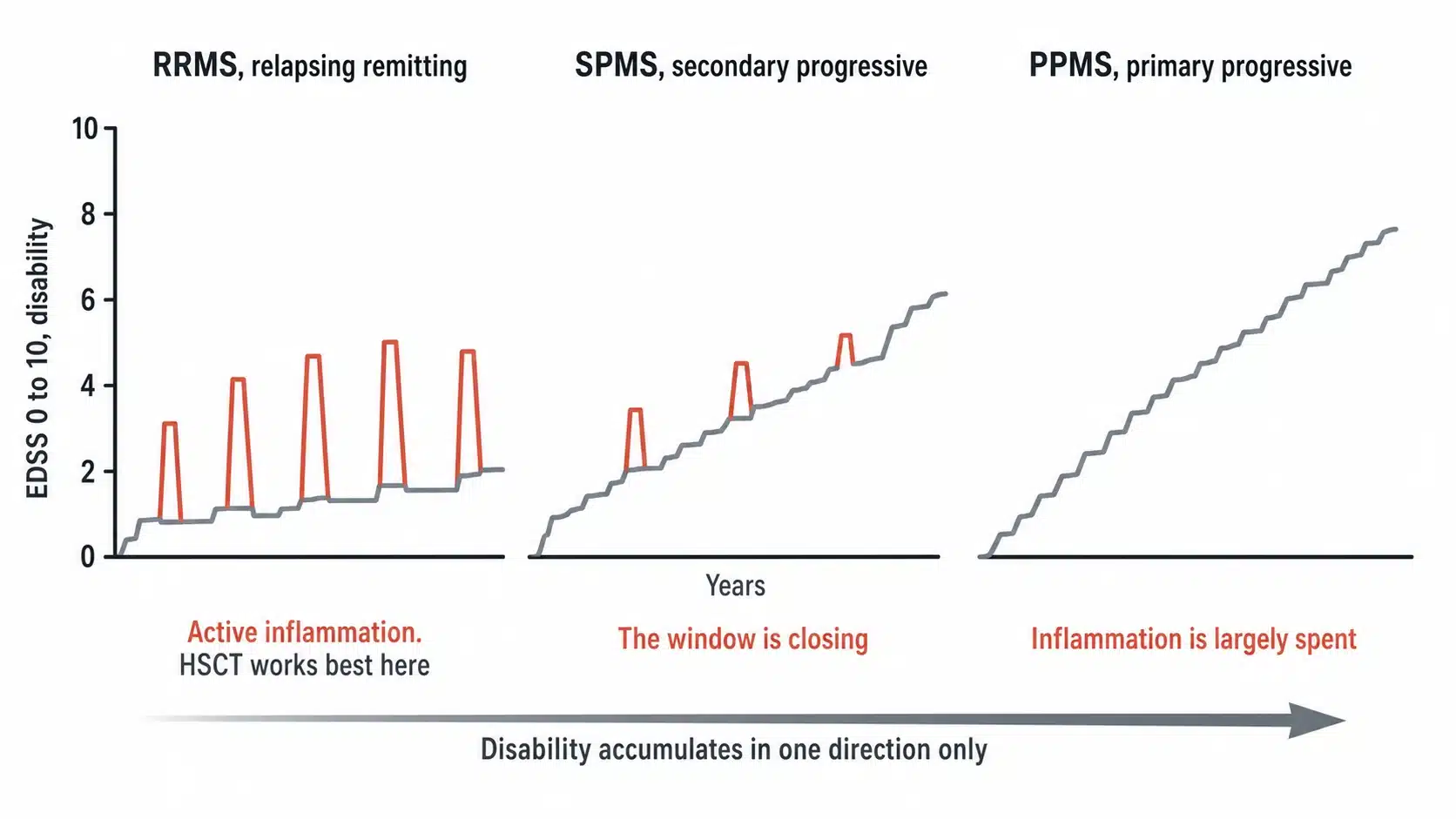
Figure 3. Relapsing remitting MS can convert to secondary progressive MS over years, while primary progressive MS declines gradually from the start. The presence of active inflammation, not the label, is what predicts benefit from HSCT.
Why Untreated MS Accumulates Disability
Untreated relapsing MS does not stand still. Each relapse carries a risk of leaving permanent deficit, and the MRI continues to accumulate lesions even in periods when the patient feels well, so-called silent progression. Over years this produces the familiar trajectory: a cane, then a walking frame, then a wheelchair, alongside bladder dysfunction, cognitive decline and fatigue. The window in which the disease is inflammatory, and therefore treatable at its root, is finite. Every relapse that is allowed to happen is a chance for inflammation to convert into damage that no later treatment can reverse. That is the clinical case for treating early and treating hard.
Standard MS Disease-Modifying Therapy, and Its Ceiling
The mainstay of MS care is disease-modifying therapy, or DMT, a family of drugs that reduce the frequency of relapses. They range in strength from injectables such as interferon beta and glatiramer acetate, through oral agents such as dimethyl fumarate, fingolimod and cladribine, to the high-efficacy monoclonal antibodies natalizumab, ocrelizumab and alemtuzumab.
These drugs work, and for many patients a well-chosen DMT controls the disease for years. But they share two limitations. First, they suppress or modulate the immune system continuously, which means they must be taken indefinitely, and stopping some of them can trigger a severe rebound of disease. Second, a proportion of patients continue to relapse or accumulate lesions despite even the strongest DMT. It is this group, patients with active disease that has broken through high-efficacy therapy, for whom HSCT is designed. A transplant does something no DMT does: instead of suppressing the faulty immune system month after month, it resets it once.
 Get HSCT India Brochure Emailed to you
Get HSCT India Brochure Emailed to you
Can HSCT Treat Multiple Sclerosis? What the Evidence Shows
Autologous HSCT is the most effective treatment for active relapsing MS studied in a randomised trial, and it is the only one that produces lasting remission without continuing medication. In the MIST randomised controlled trial, published in JAMA in 2019, patients with relapsing MS who continued to relapse on disease-modifying drugs were randomised to a transplant or to a switch of DMT. Disease progression struck about 6 per cent of the transplant group and roughly two thirds of those who stayed on drugs. On average, disability improved after the transplant and worsened on the medicines. It was the first randomised trial to show a stem cell transplant beating the best drugs available for MS, and it changed how the disease is understood.
The durability is now well documented. A long-term outcome study in JAMA Neurology reported that a majority of transplanted relapsing patients remained free of any evidence of disease activity for five years, a standard, called NEDA, that high-efficacy drugs rarely sustain. The HALT-MS trial reported event-free survival close to seventy per cent at five years after a single procedure and no maintenance therapy. A meta-analysis of transplant series found that the patients who did best were younger, had relapsing rather than progressive disease, and had a shorter disease duration. A real-world series of 507 patients confirmed these outcomes outside the controlled trial setting. At HSCT Hospital India we have treated more than 1,500 international patients using the non-myeloablative protocol pioneered by Professor Richard K. Burt, and we see a relapse-free rate of about 87 per cent at four years. The patients in the stories further down this page are real people who came to us with active MS and got their lives back.
The numbers, in one place: in the randomised trial, disease progression hit about 6 per cent of transplanted patients against roughly two thirds on drugs; most transplanted patients reach lasting remission with no evidence of disease activity, a result the strongest drugs rarely hold; and our own four-year relapse-free rate is about 87 per cent. HSCT works, and it works best in exactly the patient this page is written for: active, relapsing, and treated before the disease has done its lasting damage.
| Study | Population | Key finding |
|---|---|---|
| MIST, JAMA 2019 | Relapsing MS failing DMT | HSCT superior to continued disease-modifying therapy; disability improved after transplant |
| Muraro, JAMA Neurology 2017 | Long-term follow-up | Majority NEDA at five years; strongest results in relapsing disease |
| HALT-MS, Neurology 2017 | Relapsing-remitting MS | Around 70 per cent event-free at five years after one procedure, no maintenance drug |
| Sormani meta-analysis, 2017 | Pooled transplant series | Best outcomes in younger, relapsing, shorter-duration patients |
Table 2. What the principal studies of HSCT for multiple sclerosis found. Full citations link to PubMed.
How Autologous HSCT Halts the Immune Attack on Myelin
An autologous transplant uses the patient’s own haematopoietic, or blood-forming, stem cells. There is no donor and no matching, so there is no risk of graft-versus-host disease. It proceeds in four stages.
- Mobilisation. A short course of chemotherapy and a growth factor coax stem cells out of the bone marrow and into the bloodstream.
- Harvest, or leukapheresis. The stem cells are collected from the blood through a machine, similar to a blood donation, and then cryopreserved, meaning frozen and stored.
- Conditioning. This is the therapeutic core. Immunosuppressive conditioning chemotherapy is given to deplete the autoreactive immune cells that have been attacking the myelin. The dose is non-myeloablative, meaning it is calibrated to reset the immune system rather than to destroy the bone marrow, which is the approach with the best safety record in autoimmune disease.
- Reinfusion. The patient’s own stored stem cells are returned through a drip. They re-engraft in the marrow and rebuild a new immune system that has, in effect, forgotten its attack on myelin.
The goal is not to repair damage that is already done. It is to remove the immune attack so that no new damage is inflicted, giving the nervous system the stable environment it needs.
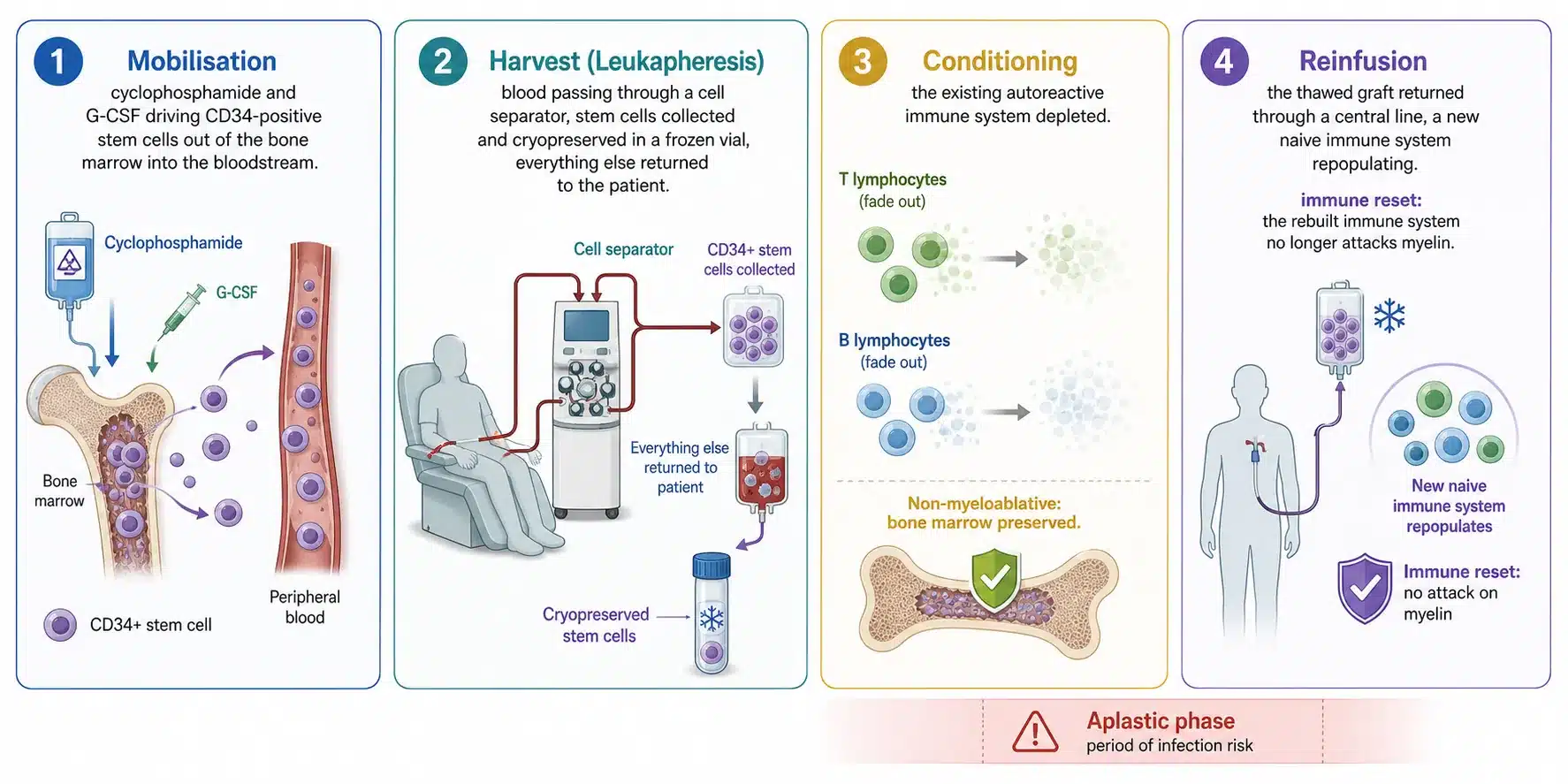
Figure 4. The four stages of autologous HSCT for MS: mobilisation, harvest, conditioning and reinfusion. There is no donor, so there is no graft-versus-host disease.
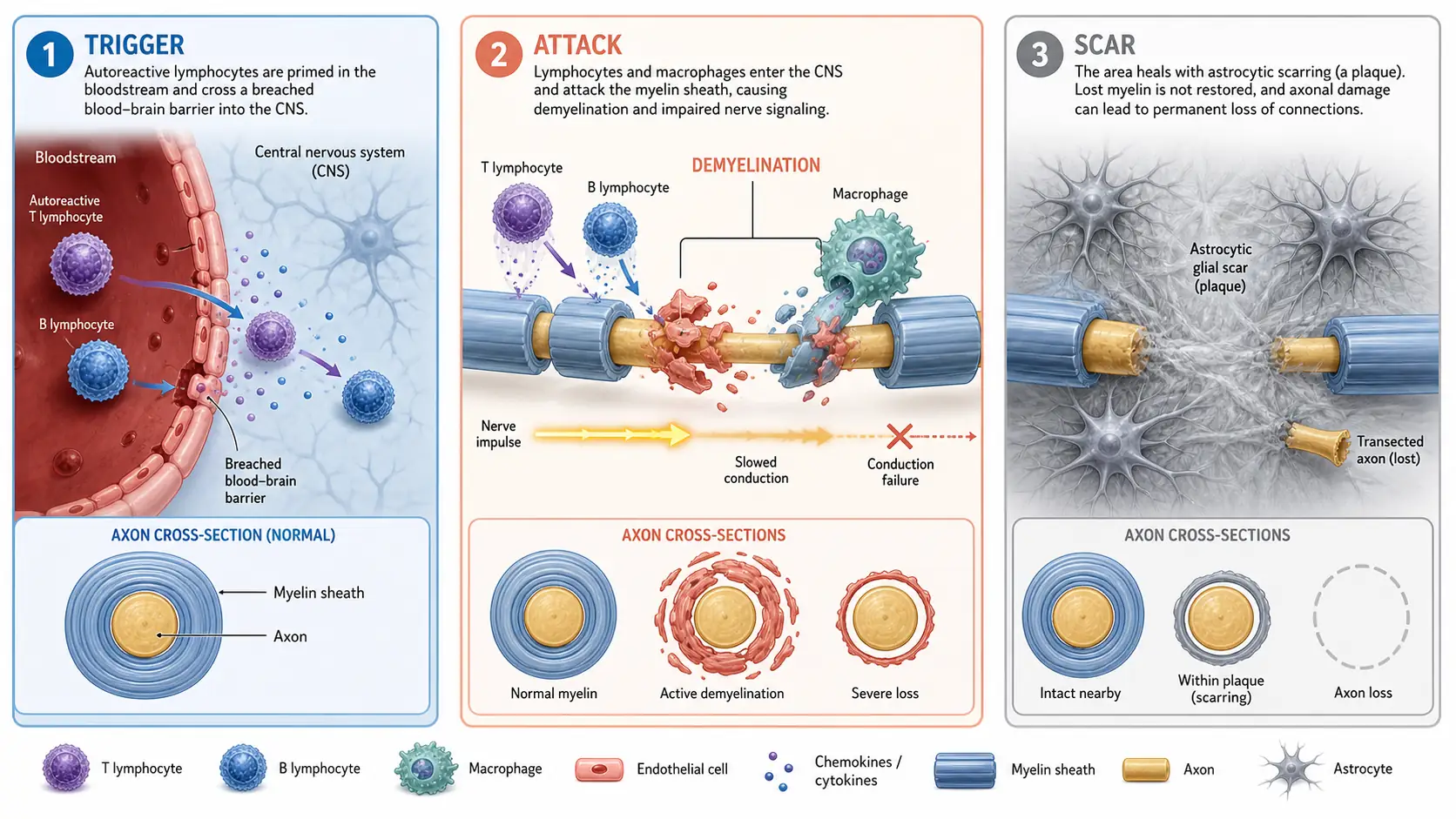
Figure 5. HSCT does not repair damage already done. It removes the immune attack on myelin, so no new damage is inflicted and the nervous system has a stable environment in which to settle.
The Thirty-Day Inpatient Stay for an MS Transplant
At HSCT Hospital India the entire treatment is done as an inpatient over roughly thirty days, and understanding the timeline removes much of the fear. The first days are the harvest and the start of conditioning. In the second week, after conditioning, the immune system reaches its lowest point, the aplastic phase, when the white cell count is very low and the risk of infection is at its height. This is the period that determines the safety of the whole procedure, and it is spent in a private room with triple HEPA air filtration and 24 hour nursing, so that any fever is caught and treated at once. In the third and fourth weeks the reinfused stem cells engraft, the blood counts recover, and the patient is prepared for discharge. There is no follow-up chemotherapy after leaving the hospital.
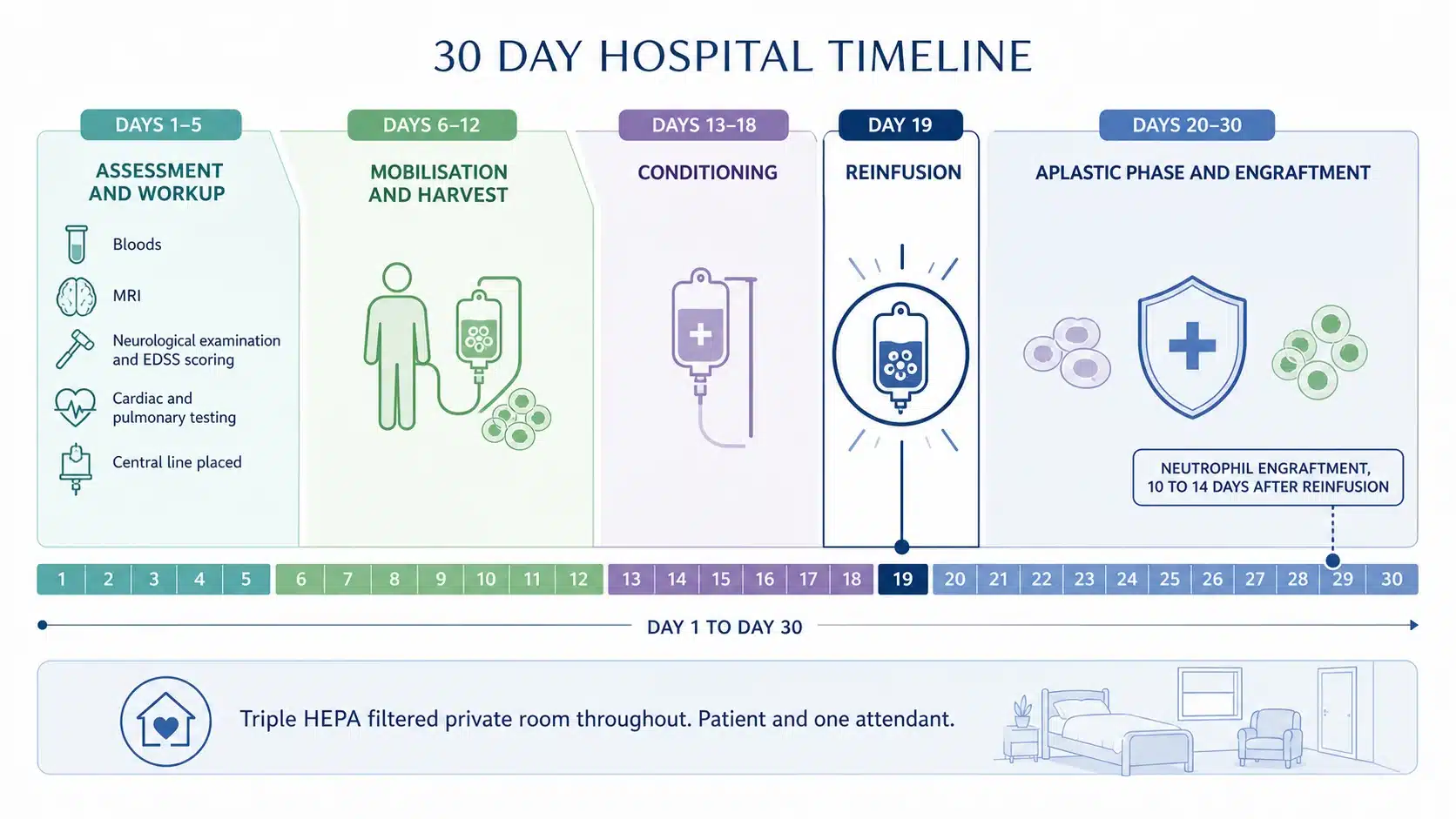
Figure 6. The 30 day inpatient programme, from harvest and conditioning through the aplastic phase to engraftment and discharge. The two weeks after conditioning are when the infection risk is real, which is why the whole stay is inpatient.
The Risks of HSCT in MS, Weighed Against the Alternative
HSCT is a serious treatment, and its risk is real, well understood, and concentrated into a single known window. The main risk is infection in the two weeks after conditioning, when the immune system is at its lowest, and it is managed by running the whole programme as an inpatient in a HEPA-filtered transplant unit with 24 hour nursing, not on an outpatient basis. The other effects are the temporary ones of chemotherapy, such as nausea, mouth soreness and hair loss, and a possible effect on fertility, which is discussed and planned for beforehand. In modern non-myeloablative programmes for MS, transplant-related mortality in suitable patients is low, and it has kept falling as selection and supportive care have improved. Weighed against what untreated relapsing MS does to a person over a lifetime, it is a risk many patients are ready to take, and it is a decision made together, formally, before anything begins.
Should I Choose HSCT or Stay on Disease-Modifying Drugs?
The real decision for most patients is not HSCT versus nothing, it is HSCT versus continuing on drugs. The two are different in kind. A DMT suppresses the immune system continuously and must be taken for life; if it is working and well tolerated, there may be no reason to change. HSCT resets the immune system once and, in the patients who respond, ends the need for ongoing therapy altogether.
The case for a transplant is strongest where drugs are failing: where relapses or new MRI lesions continue despite a high-efficacy DMT, where the disease is aggressive and the patient is young, or where the side effects and rebound risk of lifelong immunosuppression are themselves a burden. The case for staying on drugs is strongest where a DMT is achieving full control with no breakthrough activity. This is the conversation a formal transplant evaluation exists to have, and it is decided on your MRI activity, your relapse history and your EDSS, not on a general rule.
Can Multiple Sclerosis Be Cured?
Autologous HSCT offers what no drug for MS can: long-term, drug-free remission. Most transplanted patients with active relapsing disease stay free of disease activity for years after a single treatment, off all medication. For a younger patient with aggressive, active MS, that is not a new prescription, it is a new trajectory.
Doctors are careful with the word cure, because MS can leave damage behind and no medicine is licensed as one. But drug-free remission is what patients come to us for, and it is what the evidence and our own results show they get. HSCT stops the immune attack; it cannot regrow nerve fibres already lost, and that is exactly why the time to act is while the disease is still active, before that damage is done. Even the minority who relapse rarely return to where they started, and drugs that had stopped working often work again afterwards. If your MS is active, the risk is in waiting, not in the treatment.
Who Is a Candidate for MS HSCT, and How We Judge It
HSCT is not the right fit for every person with MS, and we would never suggest it was. Everything on this page converges on a single eligibility principle: the patient who benefits is the patient whose disability is still being driven by active inflammation, not by accumulated degeneration. In practice, our multi-disciplinary team assesses:
- A confirmed diagnosis of MS on the McDonald criteria
- Active, inflammatory disease, shown by recent relapses or new or enhancing lesions on MRI
- Relapsing-remitting disease, or secondary progressive disease that still shows inflammatory activity
- An EDSS score generally at or below 6.5
- Insufficient response to, or intolerance of, high-efficacy disease-modifying therapy
- Adequate heart, lung, liver and kidney function, and general fitness for the procedure
A patient with long-standing progressive MS, a high EDSS and no inflammatory activity is the patient for whom a transplant offers least, and we will say so. Turning away a patient we cannot help means a lost booking for us. Treating a patient we cannot help costs that person far more. The same rigorous selection applies to the other autoimmune conditions we treat, including stiff person syndrome,myositis, CIDP, NMOSD and myasthenia gravis.
 Request a Call Back
Request a Call BackMS HSCT Cost in India, Set Beside Other Countries
At HSCT Hospital India the entire transplant is offered as one all-inclusive package costing 30,000 US dollars. It bundles thirty days of inpatient care for the patient and one attendant, a deluxe private room with triple HEPA air filtration, and every clinical charge that follows: doctors’ fees, tests, medicines, consumables, neuro-physiotherapy, food and laundry for both, and airport transfers. The same non-myeloablative treatment costs far more elsewhere, chiefly because a hospital bed and a specialist’s salary cost less in India, not because the protocol is different.
| Country | Typical all-inclusive cost | Care model |
|---|---|---|
| India (HSCT Hospital India) | $30,000 | Fully inpatient, JCI-USA accredited, HEPA-filtered BMT room |
| Russia (Pirogov Centre, Moscow) | $40,000 to $45,000 | Inpatient |
| Mexico (Clinica Ruiz) | Around $54,500 | Largely outpatient |
| USA | $150,000 to $200,000 | Inpatient, usually only inside a clinical trial |
Table 3. Indicative cost of HSCT for MS by country. A full, sourced comparison is set out in our HSCT cost by country guide.
Frequently Asked Questions About HSCT for Multiple Sclerosis
Does HSCT stop multiple sclerosis?
In active, relapsing MS, yes: the MIST randomised trial and long-term follow-up studies show that HSCT halts relapses and new lesion formation in the great majority of appropriately selected patients, and does so without any continuing drug. It stops the inflammatory attack; it does not reverse nerve damage already sustained, which is why it is most effective when done early.
Is HSCT better than disease-modifying drugs for MS?
For patients who keep relapsing despite high-efficacy DMTs, the randomised evidence shows HSCT is more effective than switching to another drug. For patients whose disease is fully controlled on a DMT, a transplant may add little. The decision depends on whether your disease is still active.
Who is a good candidate for HSCT for MS?
Younger patients with relapsing-remitting MS, active inflammation on MRI, a shorter disease duration, an EDSS at or below 6.5, and disease that has broken through strong drug therapy. These are the features associated with the best outcomes.
Is HSCT for MS safe?
It carries real risk, concentrated in the two-week aplastic phase when the immune system is at its lowest. That is why the whole thirty-day programme at HSCT Hospital India is inpatient, in a HEPA-filtered BMT room with 24 hour nursing, in a JCI-USA accredited hospital. Transplant-related mortality in modern non-myeloablative programmes for selected patients is low.
How long does HSCT for MS take?
About thirty days in hospital, followed by a recovery period at home over the following months as the new immune system matures. There is no follow-up chemotherapy.
Will my MS symptoms improve after HSCT?
The primary goal is to stop new damage. Many patients also see improvement in symptoms driven by recent inflammation, particularly fatigue and relapse-related deficits, while damage that is already fixed is less likely to reverse.
Do I need chemotherapy for life after HSCT?
No. The non-myeloablative protocol conditions the immune system once. After engraftment, the treatment is complete and no maintenance chemotherapy is required.
Can HSCT help progressive MS?
It can help secondary progressive MS only where active inflammation is still present. Where progression is driven purely by degeneration, with no relapses and no new lesions, a transplant offers little.
How much does HSCT for MS cost in India?
The all-inclusive package is 30,000 US dollars, covering thirty days in hospital for the patient and one attendant, with all fees, tests, medicines, physiotherapy, food and airport transfers included.
How soon can I be treated?
Weeks, not years. In most national health systems HSCT for MS is available only inside a clinical trial, if at all. Because every relapse can leave permanent damage, the waiting time is not administrative, it is clinical.
What Is the Next Step?
Nothing on this page can tell you whether HSCT is right for you. That question is answered by a formal transplant evaluation, which reviews your MRI activity, your relapse history and your EDSS together, confirms whether your disability is still being driven by inflammation, and sets out the fixed package cost in writing. Delivering that evaluation is precisely our work, and the section below introduces the centre where it is carried out.
Get HSCT India Brochure Emailed to you. Consult Top HSCT Doctors
Send us your recent MRI scans, your neurologist reports and your EDSS score, and we will email you the HSCT information booklet with the full costed package and arrange a call with our HSCT doctors, free of charge. Click here to send your enquiry.
Why Choose HSCT Hospital India for Life Changing MS Treatment

 Complete 30 day HSCT done in hospital. Private deluxe rooms are very well served for patient and attendant comfort and equipped with HEPA Filter with Triple Level Air Filtration. No outside hospital stay avoids risk of infection during the aplastic phase, 24 x 7 nursing care and best medical attention. The advanced HSCT protocol used does not require any further chemo or treatment after leaving the hospital. Click here to get complete details
Complete 30 day HSCT done in hospital. Private deluxe rooms are very well served for patient and attendant comfort and equipped with HEPA Filter with Triple Level Air Filtration. No outside hospital stay avoids risk of infection during the aplastic phase, 24 x 7 nursing care and best medical attention. The advanced HSCT protocol used does not require any further chemo or treatment after leaving the hospital. Click here to get complete details
 International and Globally Renowned Accreditations. HSCT Hospital India is accredited by the Joint Commission International, USA, the National Accreditation Board for Hospitals and Healthcare Providers (NABH), and the National Accreditation Board for Laboratories (NABL) for processes and high quality patient care. Click here to know more
International and Globally Renowned Accreditations. HSCT Hospital India is accredited by the Joint Commission International, USA, the National Accreditation Board for Hospitals and Healthcare Providers (NABH), and the National Accreditation Board for Laboratories (NABL) for processes and high quality patient care. Click here to know more
Real Patient– Real Stories


